Field Nigel, Prah Philip, Mercer Catherine H, Rait Greta, King Michael, Cassell Jackie A, Tanton Clare, Heath Laura, Mitchell Kirstin R, Clifton Soazig, Datta Jessica, Wellings Kaye, Johnson Anne M, Sonnenberg Pam
Research Department of Infection and Population Health, UCL, London, UK.
Research Department of Primary Care and Population Health, UCL, London, UK.
BMJ Open. 2016 Mar 23;6(3):e010521. doi: 10.1136/bmjopen-2015-010521.
To examine associations between sexual behaviour, sexual function and sexual health service use of individuals with depression in the British general population, to inform primary care and specialist services.
British general population.
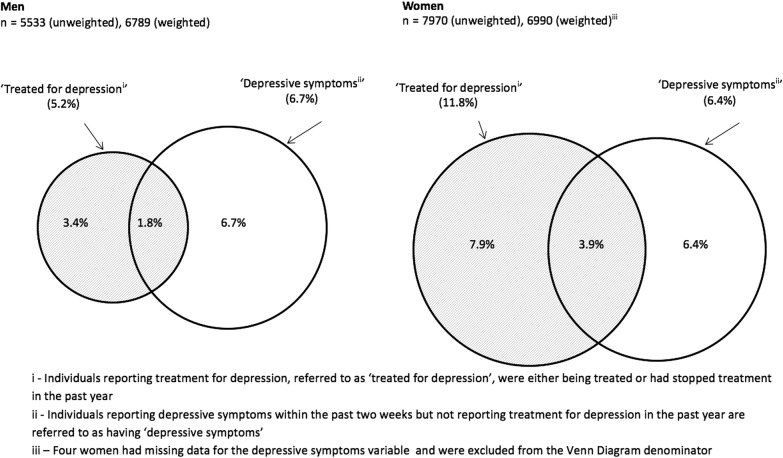
15,162 men and women aged 16-74 years were interviewed for the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3), undertaken in 2010-2012. Using age-adjusted ORs (aAOR), relative to a comparator group reporting no treatment or symptoms, we compared the sexual health of those reporting treatment for depression in the past year.
Sexual risk behaviour, sexual function, sexual satisfaction and sexual health service use.
1331 participants reported treatment for depression (5.2% men; 11.8% women). Relative to the comparator group, treatment for depression was associated with reporting 2 or more sexual partners without condoms (men aAOR 2.07 (95% CI 1.38 to 3.10); women 2.22 (1.68 to 2.92)), and concurrent partnerships (men 1.80 (1.18 to 2.76); women 2.06 (1.48 to 2.88)), in the past year. Those reporting depression treatment were more likely to be dissatisfied with their sex lives (men 2.32 (1.74 to 3.11); women 2.30 (1.89 to 2.79)), and to score in the lowest quintile on the Natsal-sexual function measure. They were also more likely to report a recent chlamydia test (men 1.92 (1.15 to 3.20)); women (1.27 (1.01 to 1.60)), and to have sought help regarding their sex life from a healthcare professional (men 2.92 (1.98 to 4.30); women (2.36 (1.83 to 3.04)), most commonly from a family doctor. Women only were more likely to report attending a sexual health clinic (1.91 (1.42 to 2.58)) and use of emergency contraception (1.98 (1.23 to 3.19)). Associations were broadly similar for individuals with depressive symptoms but not reporting treatment.
Depression, measured by reported treatment, was strongly associated with sexual risk behaviours, reduced sexual function and increased use of sexual health services, with many people reporting help doing so from a family doctor. The sexual health of depressed people needs consideration in primary care, and mental health assessment might benefit people attending sexual health services.
研究英国普通人群中抑郁症患者的性行为、性功能与性健康服务利用之间的关联,以为初级保健和专科服务提供参考。
英国普通人群。
在2010 - 2012年进行的第三次全国性态度和生活方式调查(Natsal - 3)中,对15162名年龄在16 - 74岁的男性和女性进行了访谈。相对于报告未接受治疗或无相关症状的对照组,我们使用年龄调整后的比值比(aAOR),比较了过去一年中报告接受抑郁症治疗者的性健康状况。
性风险行为、性功能、性满意度和性健康服务利用情况。
1331名参与者报告接受过抑郁症治疗(男性5.2%;女性11.8%)。相对于对照组,抑郁症治疗与过去一年中报告有2个或更多未使用避孕套的性伴侣相关(男性aAOR为2.07(95%置信区间1.38至3.10);女性为2.22(1.68至2.92)),以及同时存在多个性伴侣相关(男性1.80(1.18至2.76);女性2.06(1.48至2.88))。报告接受抑郁症治疗的人对其性生活更有可能不满意(男性2.32(1.74至3.11);女性2.30(1.89至2.79)),并且在Natsal性功能测量中得分处于最低五分位数。他们也更有可能报告最近进行过衣原体检测(男性1.92(1.15至3.20);女性1.27(1.01至1.60)),以及曾就其性生活向医疗保健专业人员寻求帮助(男性2.92(1.98至4.30);女性2.36(1.83至3.04)),最常见的是向家庭医生求助。仅女性更有可能报告去过性健康诊所(1.91(1.42至2.58))和使用过紧急避孕措施(1.98(从1.23至3.19))。对于有抑郁症状但未报告接受治疗的个体,关联情况大致相似。
通过报告接受治疗来衡量,抑郁症与性风险行为、性功能降低以及性健康服务利用增加密切相关,许多人报告从家庭医生处获得了相关帮助。初级保健中需要考虑抑郁症患者的性健康,而心理健康评估可能会使前往性健康服务机构就诊的人受益。