Hannukainen J C, Lautamäki R, Mari A, Pärkkä J P, Bucci M, Guzzardi M A, Kajander S, Tuokkola T, Knuuti J, Iozzo P
Turku PET Center (J.C.H., R.L., J.P.P., M.B., S.K., T.T., J.K., P.I.), University of Turku, 20014 Turku, Finland; Heart Center (R.L.), Turku University Hospital, 20520 Turku, Finland; Institute of Neuroscience (A.M.), National Research Council, 35127 Padua, Italy; and Institute of Clinical Physiology (M.A.G., P.I.), National Research Council, 56124 Pisa, Italy.
J Clin Endocrinol Metab. 2016 Jul;101(7):2701-10. doi: 10.1210/jc.2015-4091. Epub 2016 Apr 5.
Insulin resistance, β-cell dysfunction, and ectopic fat deposition have been implicated in the pathogenesis of coronary artery disease (CAD) and type 2 diabetes, which is common in CAD patients. We investigated whether CAD is an independent predictor of these metabolic abnormalities and whether this interaction is influenced by superimposed myocardial ischemia.
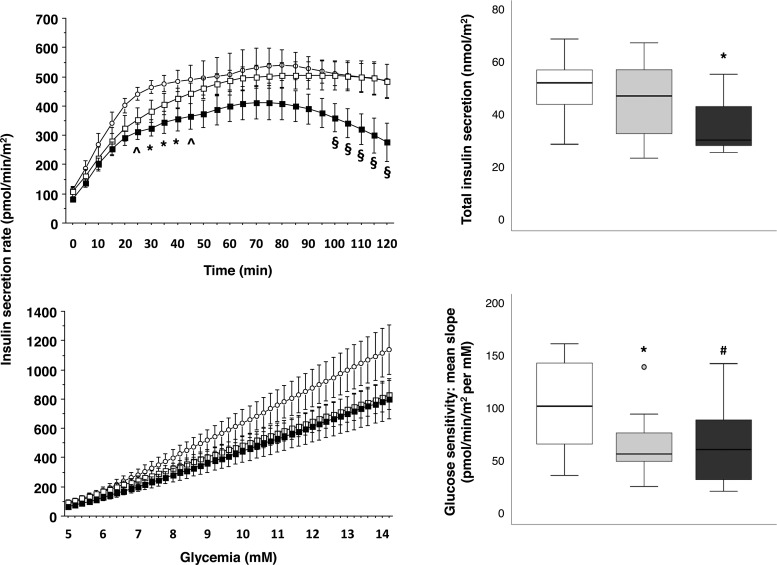
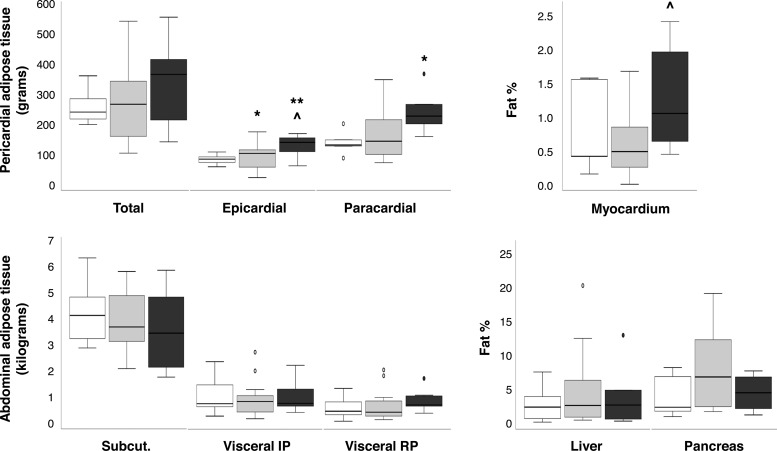
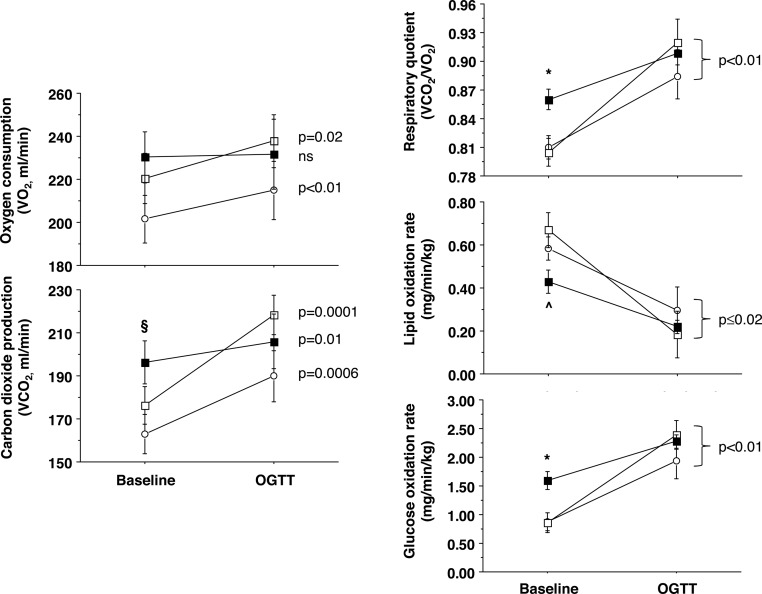
We studied CAD patients with (n = 8) and without (n = 14) myocardial ischemia and eight non-CAD controls. Insulin sensitivity and secretion and substrate oxidation were measured during fasting and oral glucose tolerance testing. We used magnetic resonance imaging/spectroscopy, positron emission and computerized tomography to characterize CAD, cardiac function, pericardial and abdominal adipose tissue, and myocardial, liver, and pancreatic triglyceride contents. Ischemic CAD was characterized by elevated oxidative glucose metabolism and a proportional decline in β-cell insulin secretion and reduction in lipid oxidation. Cardiac function was preserved in CAD groups, whereas cardiac fat depots were elevated in ischemic CAD compared to non-CAD subjects. Liver and pancreatic fat contents were similar in all groups and related with surrounding adipose masses or systemic insulin sensitivity.
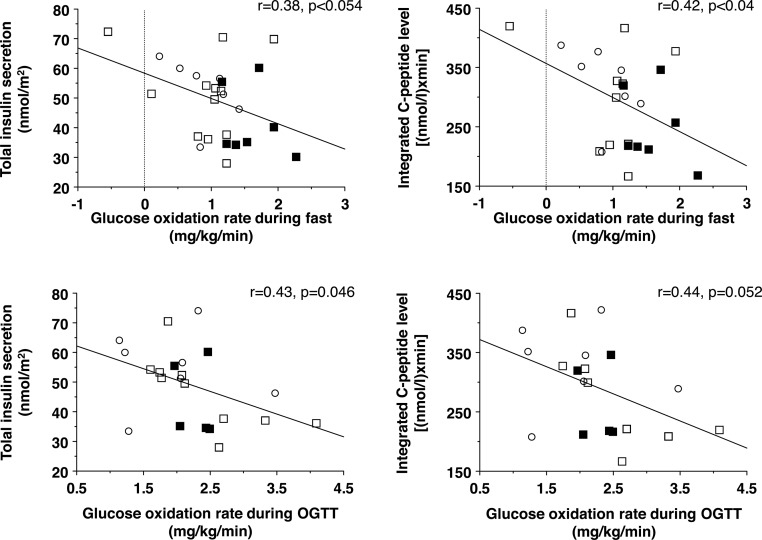
In ischemic CAD patients, glucose oxidation is enhanced and correlates inversely with insulin secretion. This can be seen as a mechanism to prevent glucose lowering because glucose is required in oxygen-deprived tissues. On the other hand, the accumulation of cardiac triglycerides may be a physiological adaptation to the limited fatty acid oxidative capacity. Our results underscore the urgent need of clinical trials that define the optimal/safest glycemic range in situations of myocardial ischemia.
胰岛素抵抗、β细胞功能障碍和异位脂肪沉积与冠状动脉疾病(CAD)和2型糖尿病的发病机制有关,2型糖尿病在CAD患者中很常见。我们研究了CAD是否是这些代谢异常的独立预测因素,以及这种相互作用是否受叠加心肌缺血的影响。
我们研究了有(n = 8)和无(n = 14)心肌缺血的CAD患者以及8名非CAD对照者。在空腹和口服葡萄糖耐量试验期间测量胰岛素敏感性、分泌和底物氧化。我们使用磁共振成像/光谱、正电子发射断层扫描和计算机断层扫描来表征CAD、心脏功能、心包和腹部脂肪组织以及心肌、肝脏和胰腺甘油三酯含量。缺血性CAD的特征是氧化葡萄糖代谢升高、β细胞胰岛素分泌成比例下降以及脂质氧化减少。CAD组心脏功能得以保留,而与非CAD受试者相比,缺血性CAD患者的心脏脂肪储存增加。所有组的肝脏和胰腺脂肪含量相似,且与周围脂肪块或全身胰岛素敏感性相关。
在缺血性CAD患者中,葡萄糖氧化增强且与胰岛素分泌呈负相关。这可被视为一种防止血糖降低的机制,因为缺氧组织需要葡萄糖。另一方面,心脏甘油三酯的积累可能是对有限脂肪酸氧化能力的一种生理适应。我们的结果强调了开展临床试验的迫切需求,这些试验应确定心肌缺血情况下的最佳/最安全血糖范围。