Wardliparingga Aboriginal Research Unit, South Australian Health and Medical Research Institute, Adelaide, Australia.
Johanna Briggs Institute, Faculty of Health Sciences, University of Adelaide, Adelaide, Australia.
BMC Health Serv Res. 2016 Apr 6;16:119. doi: 10.1186/s12913-016-1363-0.
Indigenous peoples in Australia, New Zealand and Canada carry a greater burden of chronic kidney disease (CKD) than the general populations in each country, and this burden is predicted to increase. Given the human and economic cost of dialysis, understanding how to better manage CKD at earlier stages of disease progression is an important priority for practitioners and policy-makers. A systematic review of mixed evidence was undertaken to examine the evidence relating to the effectivness, cost-effectiveness and acceptability of chronic kidney disease management programs designed for Indigenous people, as well as barriers and enablers of implementation of such programs.
Published and unpublished studies reporting quantitative and qualitative data on health sector-led management programs and models of care explicitly designed to manage, slow progression or otherwise improve the lives of Indigenous people with CKD published between 2000 and 2014 were considered for inclusion. Data on clinical effectiveness, ability to self-manage, quality of life, acceptability, cost and cost-benefit, barriers and enablers of implementation were of interest. Quantitative data was summarized in narrative and tabular form and qualitative data was synthesized using the Joanna Briggs Institute meta-aggregation approach.
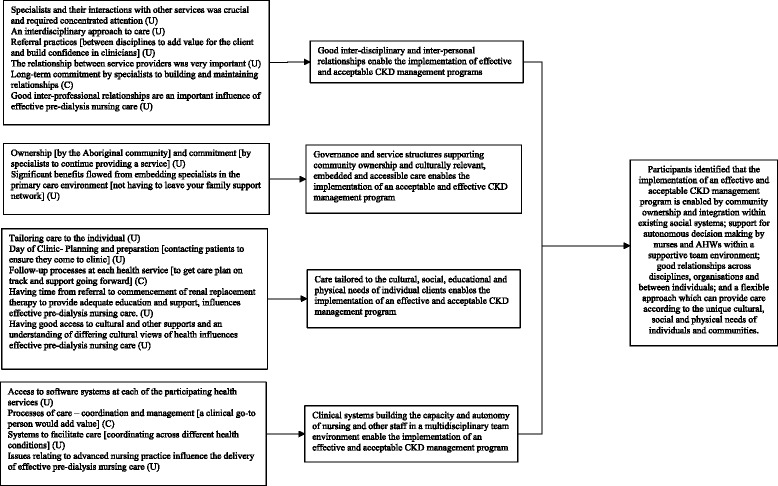
Ten studies were included. Six studies provided evidence of clinical effectiveness of CKD programs designed for Indigenous people, two provided evidence of cost and cost-effectiveness of a CKD program, and two provided qualitative evidence of barriers and enablers of implementation of effective and/or acceptable CKD management programs. Common features of effective and acceptable programs were integration within existing services, nurse-led care, intensive follow-up, provision of culturally-appropriate education, governance structures supporting community ownership, robust clinical systems supporting communication and a central role for Indigenous Health Workers.
Given the human cost of dialysis and the growing population of people living with CKD, there is an urgent need to draw lessons from the available evidence from this and other sources, including studies in the broader population, to better serve this population with programs that address the barriers to receiving high-quality care and improve quality of life.
澳大利亚、新西兰和加拿大的原住民所患慢性肾脏病(CKD)的负担比各自国家的一般人群更重,预计这一负担还会增加。鉴于透析带来的人力和经济成本,了解如何在疾病进展的早期阶段更好地管理 CKD,是从业者和决策者的一项重要优先事项。对混合证据进行了系统回顾,以检查针对原住民设计的 CKD 管理方案的有效性、成本效益和可接受性方面的证据,以及这些方案实施的障碍和推动因素。
纳入了 2000 年至 2014 年间发表的关于卫生部门主导的管理方案和专门设计用于管理、减缓进展或改善 CKD 原住民生活的护理模式的定量和定性数据的已发表和未发表的研究报告。关注的是临床效果、自我管理能力、生活质量、可接受性、成本和成本效益、实施的障碍和推动因素。定量数据以叙述和表格形式进行总结,定性数据采用乔安娜·布里格斯研究所元聚合方法进行综合。
纳入了 10 项研究。6 项研究提供了针对原住民设计的 CKD 方案的临床效果证据,2 项研究提供了 CKD 方案的成本和成本效益证据,2 项研究提供了有效和/或可接受的 CKD 管理方案实施的障碍和推动因素的定性证据。有效的和可接受的方案的共同特点是纳入现有的服务,护士主导的护理,强化随访,提供文化适宜的教育,支持社区所有权的治理结构,支持沟通的稳健临床系统,以及原住民卫生工作者的核心作用。
鉴于透析带来的人力成本和不断增加的 CKD 患者人群,迫切需要从这一来源以及其他来源(包括更广泛人群的研究)的现有证据中吸取经验教训,制定出解决接受高质量护理障碍的方案,提高生活质量,更好地为这一人群提供服务。