Mojoli Francesco, Iotti Giorgio Antonio, Torriglia Francesca, Pozzi Marco, Volta Carlo Alberto, Bianzina Stefania, Braschi Antonio, Brochard Laurent
Anesthesia and Intensive Care, Emergency Department, Fondazione IRCCS Policlinico S. Matteo, Pavia, Italy.
Anesthesia, Intensive Care and Pain Therapy, Department of Clinical, Surgical, Diagnostic and Pediatric Sciences, University of Pavia, Pavia, Italy.
Crit Care. 2016 Apr 11;20:98. doi: 10.1186/s13054-016-1278-5.
Esophageal pressure (Pes) can provide information to guide mechanical ventilation in acute respiratory failure. However, both relative changes and absolute values of Pes can be affected by inappropriate filling of the esophageal balloon and by the elastance of the esophagus wall. We evaluated the feasibility and effectiveness of a calibration procedure consisting in optimization of balloon filling and subtraction of the pressure generated by the esophagus wall (Pew).
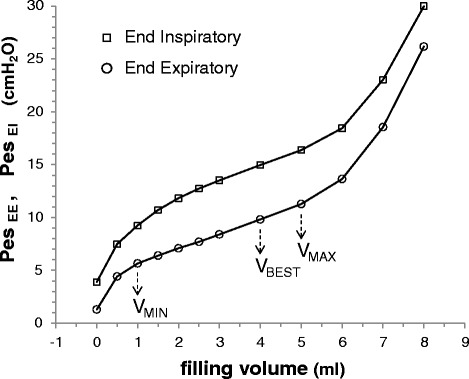
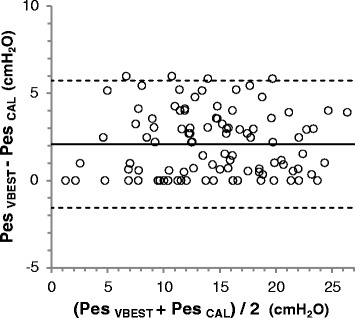
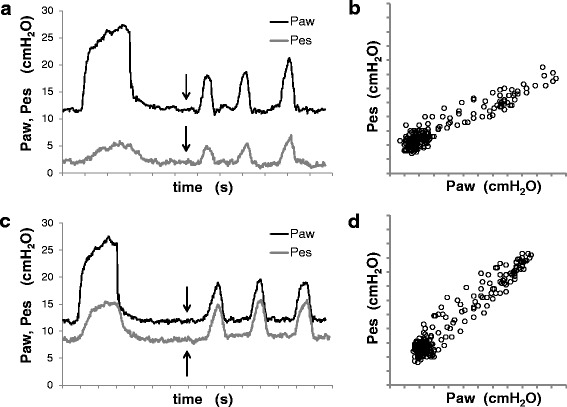
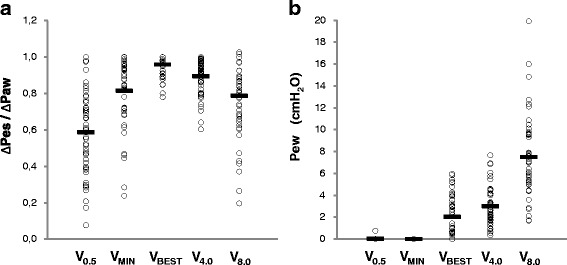
An esophageal balloon was progressively filled in 36 patients under controlled mechanical ventilation. VBEST was the filling volume associated with the largest tidal increase of Pes. Esophageal wall elastance was quantified and Pew was computed at each filling volume. Different filling strategies were compared by performing a validation occlusion test.
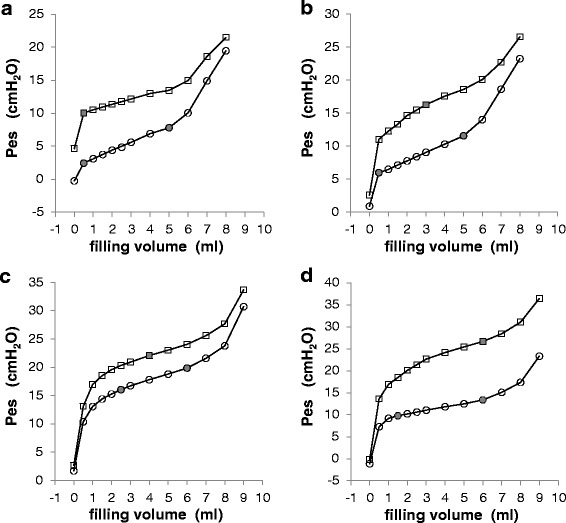
Fifty series of measurements were performed. VBEST was 3.5 ± 1.9 ml (range 0.5-6.0). Esophagus elastance was 1.1 ± 0.5 cmH2O/ml (0.3-3.1). Both Pew and the result of the occlusion test differed among filling strategies. At filling volumes of 0.5, VBEST and 4.0 ml respectively, Pew was 0.0 ± 0.1, 2.0 ± 1.9, and 3.0 ± 1.7 cmH2O (p < 0.0001), whereas the occlusion test was satisfactory in 22%, 98%, and 88% of cases (p < 0.0001).
Under mechanical ventilation, an increase of balloon filling above the conventionally recommended low volumes warrants complete transmission of Pes swings, but is associated with significant elevation of baseline. A simple calibration procedure allows finding the filling volume associated with the best transmission of tidal Pes change and subtracting the associated baseline artifact, thus making measurement of absolute values of Pes reliable.
食管压力(Pes)可为急性呼吸衰竭时机械通气的调整提供依据。然而,食管球囊充盈不当以及食管壁弹性均可影响Pes的相对变化和绝对值。我们评估了一种校准程序的可行性和有效性,该程序包括优化球囊充盈以及减去食管壁产生的压力(Pew)。
对36例接受控制机械通气的患者逐步充盈食管球囊。VBEST是与Pes潮气量最大增加相关的充盈量。对食管壁弹性进行定量,并计算每个充盈量下的Pew。通过进行验证性闭塞试验比较不同的充盈策略。
共进行了50组测量。VBEST为3.5±1.9 ml(范围0.5 - 6.0)。食管弹性为1.1±0.5 cmH₂O/ml(0.3 - 3.1)。不同充盈策略下的Pew和闭塞试验结果均存在差异。分别在充盈量为0.5、VBEST和4.0 ml时,Pew分别为0.0±0.1、2.0±1.9和3.0±1.7 cmH₂O(p<0.0001),而闭塞试验在22%、98%和88%的病例中结果满意(p<0.0001)。
在机械通气时,球囊充盈量超过传统推荐的低容量虽能保证Pes波动的完全传导,但会导致基线显著升高。一种简单的校准程序可找到与潮气量Pes变化最佳传导相关的充盈量,并减去相关的基线伪影,从而使Pes绝对值的测量可靠。