Asante Augustine, Price Jennifer, Hayen Andrew, Jan Stephen, Wiseman Virginia
School of Public Health and Community Medicine, University of New South Wales, Sydney, Australia.
The George Institute for Global Health, Sydney, NSW, 2000, Australia.
PLoS One. 2016 Apr 11;11(4):e0152866. doi: 10.1371/journal.pone.0152866. eCollection 2016.
Health financing reforms in low- and middle- income countries (LMICs) over the past decades have focused on achieving equity in financing of health care delivery through universal health coverage. Benefit and financing incidence analyses are two analytical methods for comprehensively evaluating how well health systems perform on these objectives. This systematic review assesses progress towards equity in health care financing in LMICs through the use of BIA and FIA.
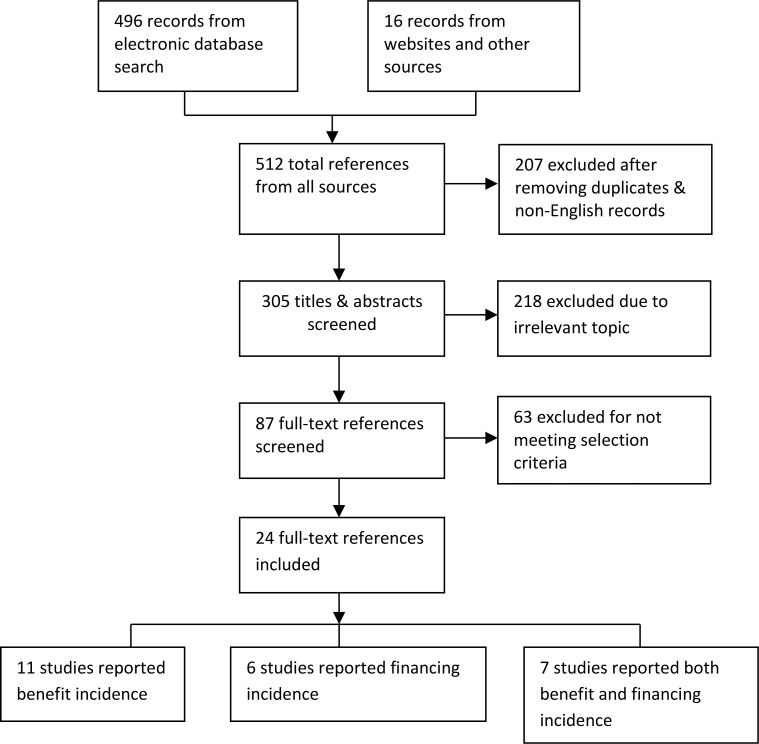
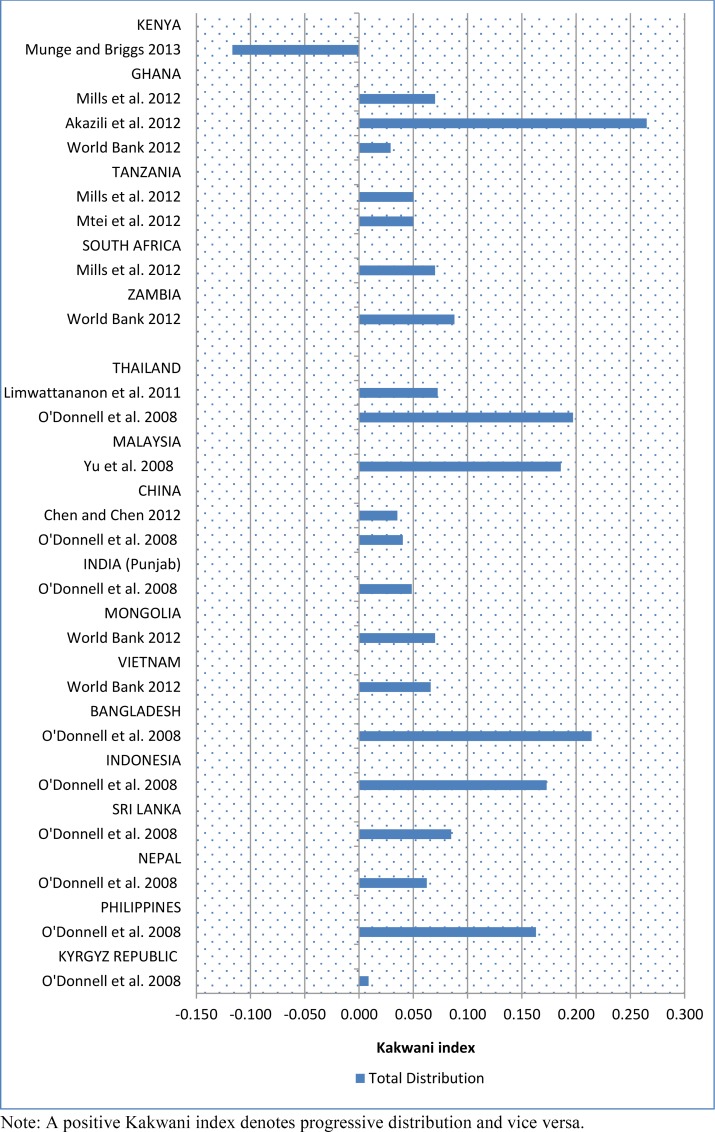
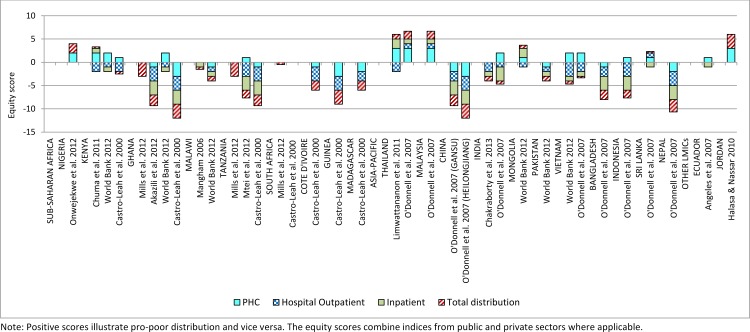
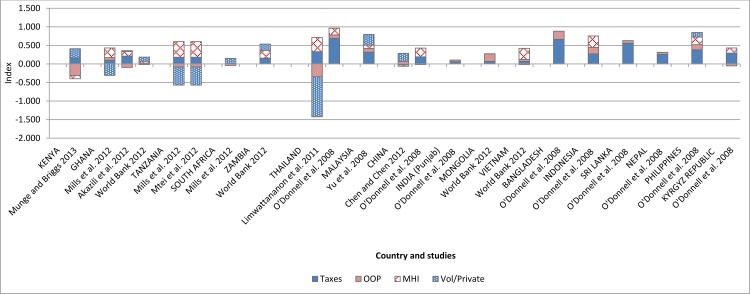
Key electronic databases including Medline, Embase, Scopus, Global Health, CinAHL, EconLit and Business Source Premier were searched. We also searched the grey literature, specifically websites of leading organizations supporting health care in LMICs. Only studies using benefit incidence analysis (BIA) and/or financing incidence analysis (FIA) as explicit methodology were included. A total of 512 records were obtained from the various sources. The full texts of 87 references were assessed against the selection criteria and 24 were judged appropriate for inclusion. Twelve of the 24 studies originated from sub-Saharan Africa, nine from the Asia-Pacific region, two from Latin America and one from the Middle East. The evidence points to a pro-rich distribution of total health care benefits and progressive financing in both sub-Saharan Africa and Asia-Pacific. In the majority of cases, the distribution of benefits at the primary health care level favoured the poor while hospital level services benefit the better-off. A few Asian countries, namely Thailand, Malaysia and Sri Lanka, maintained a pro-poor distribution of health care benefits and progressive financing.
Studies evaluated in this systematic review indicate that health care financing in LMICs benefits the rich more than the poor but the burden of financing also falls more on the rich. There is some evidence that primary health care is pro-poor suggesting a greater investment in such services and removal of barriers to care can enhance equity. The results overall suggest that there are impediments to making health care more accessible to the poor and this must be addressed if universal health coverage is to be a reality.
在过去几十年里,低收入和中等收入国家(LMICs)的卫生筹资改革一直聚焦于通过全民健康覆盖实现医疗服务筹资的公平性。受益发生率分析和筹资发生率分析是全面评估卫生系统在这些目标上表现如何的两种分析方法。本系统评价通过运用受益发生率分析(BIA)和筹资发生率分析(FIA)评估了LMICs在卫生保健筹资公平性方面的进展。
检索了包括Medline、Embase、Scopus、Global Health、CinAHL、EconLit和Business Source Premier在内的主要电子数据库。我们还检索了灰色文献,特别是支持LMICs卫生保健的主要组织的网站。仅纳入了使用受益发生率分析(BIA)和/或筹资发生率分析(FIA)作为明确方法的研究。从各种来源共获得512条记录。根据选择标准对87篇参考文献的全文进行了评估,其中24篇被判定适合纳入。24项研究中有12项来自撒哈拉以南非洲,9项来自亚太地区,2项来自拉丁美洲,1项来自中东。证据表明,撒哈拉以南非洲和亚太地区的总体医疗保健福利存在有利于富人的分配情况,且筹资具有累进性。在大多数情况下,初级卫生保健层面的福利分配有利于穷人,而医院层面的服务则使较富裕者受益。少数亚洲国家,即泰国、马来西亚和斯里兰卡,保持了有利于穷人的医疗保健福利分配和累进性筹资。
本系统评价中评估的研究表明,LMICs的卫生保健筹资使富人受益多于穷人,但筹资负担也更多地落在富人身上。有一些证据表明初级卫生保健有利于穷人,这表明对这类服务进行更多投资以及消除就医障碍可以提高公平性。总体结果表明,在使穷人更易获得医疗保健方面存在障碍,如果要实现全民健康覆盖,就必须解决这一问题。