Hunt Margie A, Sonnick Mark, Pham Hai, Regmi Rajesh, Xiong Jian-ping, Morf Daniel, Mageras Gig S, Zelefsky Michael, Zhang Pengpeng
Memorial Sloan Kettering Cancer Center.
J Appl Clin Med Phys. 2016 Mar 8;17(2):473-486. doi: 10.1120/jacmp.v17i2.5836.
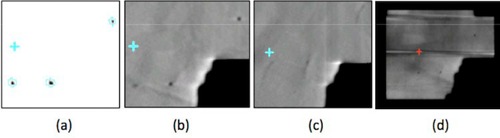
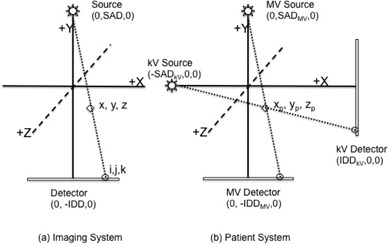
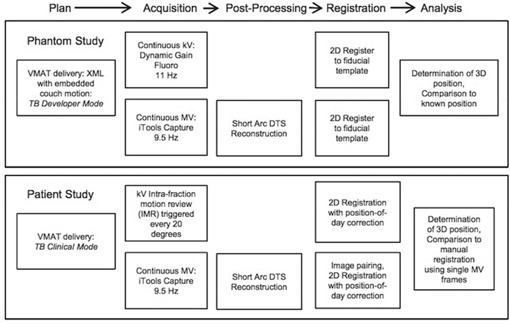
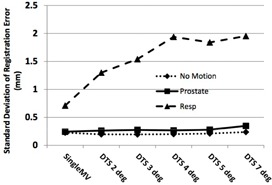
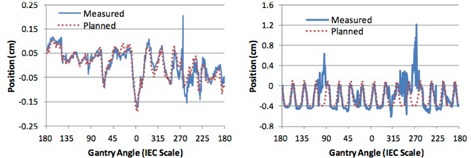
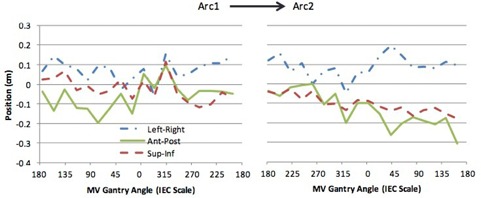
The purpose of this study was to evaluate the accuracy and clinical feasibility of a motion monitoring method employing simultaneously acquired MV and kV images during volumetric-modulated arc therapy (VMAT). Short-arc digital tomosynthesis (SA-DTS) is used to improve the quality of the MV images that are then combined with orthogonally acquired kV images to assess 3D motion. An anthropomorphic phantom with implanted gold seeds was used to assess accuracy of the method under static, typical prostatic, and respiratory motion scenarios. Automatic registra-tion of kV images and single MV frames or MV SA-DTS reconstructed with arc lengths from 2° to 7° with the appropriate reference fiducial template images was performed using special purpose-built software. Clinical feasibility was evaluated by retrospectively analyzing images acquired over four or five sessions for each of three patients undergoing hypofractionated prostate radiotherapy. The standard deviation of the registration error in phantom using MV SA-DTS was similar to single MV images for the static and prostate motion scenarios (σ = 0.25 mm). Under respiratory motion conditions, the standard deviation of the registration error increased to 0.7mm and 1.7 mm for single MV and MV SA-DTS, respectively. Registration failures were observed with the respiratory scenario only and were due to motion-induced fiducial blurring. For the three patients studied, the mean and standard deviation of the difference between automatic registration using 4° MV SA-DTS and manual registration using single MV images results was 0.07±0.52mm. The MV SA-DTS results in patients were, on average, superior to single-frame MV by nearly 1 mm - significantly more than what was observed in phantom. The best MV SA-DTS results were observed with arc lengths of 3° to 4°. Registration failures in patients using MV SA-DTS were primarily due to blockage of the gold seeds by the MLC. The failure rate varied from 2% to 16%. Combined MV SA-DTS and kV imaging is feasible for intratreatment motion monitoring during VMAT of anatomic sites where limited motion is expected, and improves registration accuracy compared to single MV/kV frames. To create a clinically robust technique, further improvements to ensure visualization of fiducials at the desired control points without degradation of the treatment plan are needed.
本研究的目的是评估在容积调强弧形放疗(VMAT)期间采用同时采集的兆伏(MV)和千伏(kV)图像的运动监测方法的准确性和临床可行性。短弧数字断层合成(SA-DTS)用于提高MV图像的质量,然后将其与正交采集的kV图像相结合以评估三维运动。使用植入金种子的人体模型来评估该方法在静态、典型前列腺运动和呼吸运动情况下的准确性。使用专门构建的软件对kV图像与单帧MV图像或使用2°至7°弧长重建的MV SA-DTS进行自动配准,并以适当的参考基准模板图像为参照。通过回顾性分析三名接受大分割前列腺放疗的患者在四到五个疗程中采集的图像来评估临床可行性。在静态和前列腺运动情况下,使用MV SA-DTS的人体模型中配准误差的标准差与单帧MV图像相似(σ = 0.25毫米)。在呼吸运动条件下,单帧MV和MV SA-DTS的配准误差标准差分别增加到0.7毫米和1.7毫米。仅在呼吸情况下观察到配准失败,这是由于运动导致基准模糊所致。对于所研究的三名患者,使用4°MV SA-DTS自动配准与使用单帧MV图像手动配准结果之间差异的平均值和标准差为0.07±0.52毫米。患者的MV SA-DTS结果平均比单帧MV图像优近1毫米,显著高于人体模型中的观测值。弧长为3°至4°时观察到最佳的MV SA-DTS结果。使用MV SA-DTS时患者的配准失败主要是由于多叶准直器(MLC)遮挡了金种子。失败率在2%至16%之间。对于预期运动有限的解剖部位,在VMAT期间联合使用MV SA-DTS和kV成像进行治疗中运动监测是可行的,并且与单帧MV/kV图像相比提高了配准准确性。为了创建一种临床稳健的技术,需要进一步改进以确保在所需控制点处基准的可视化,同时不降低治疗计划。