Epidemiology and Cancer Statistics Group, Department of Health Sciences, University of York, YO10 5DD, UK.
Epidemiology and Cancer Statistics Group, Department of Health Sciences, University of York, YO10 5DD, UK.
Cancer Epidemiol. 2016 Jun;42:186-98. doi: 10.1016/j.canep.2016.03.011. Epub 2016 Apr 16.
Population-based information on cancer incidence, prevalence and outcome are required to inform clinical practice and research; but contemporary data are lacking for many myeloid malignancy subtypes.
Set within a socio-demographically representative UK population of ∼4 million, myeloid malignancy data (N=5231 diagnoses) are from an established patient cohort. Information on incidence, survival (relative & overall), transformation/progression, and prevalence is presented for >20 subtypes.
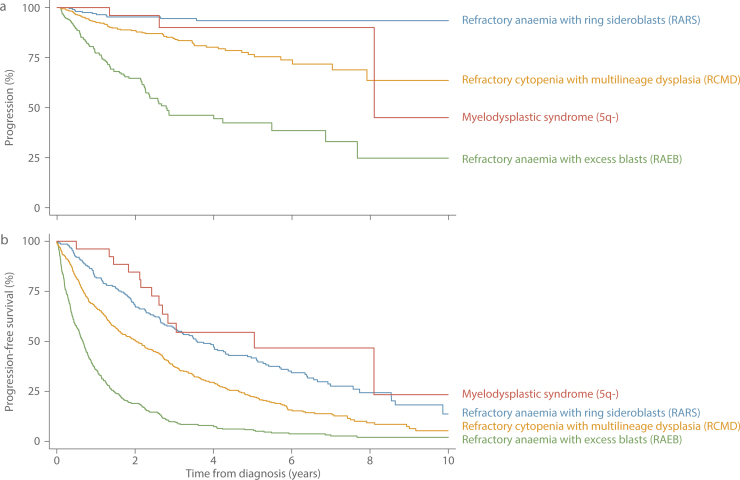
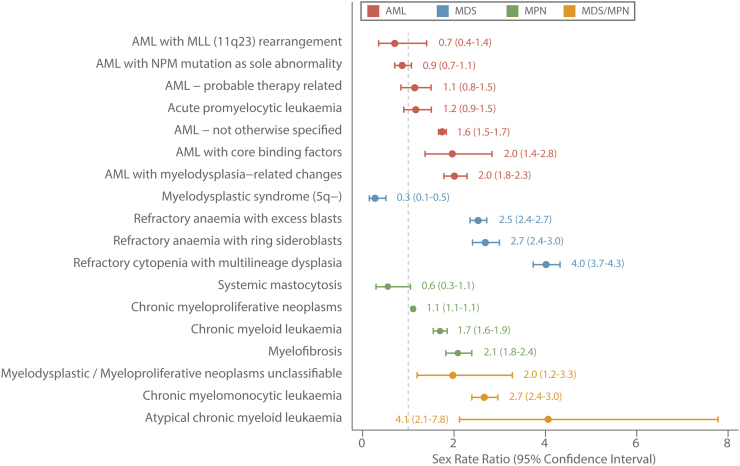
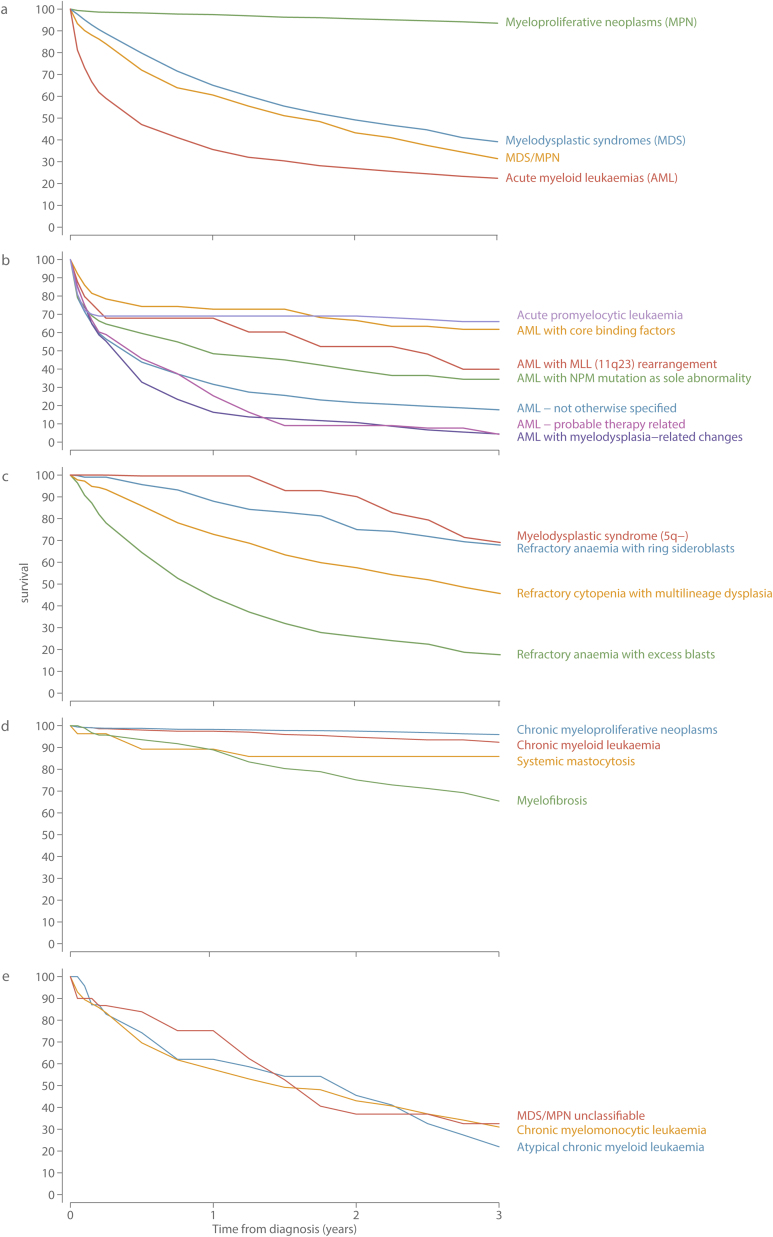
The median diagnostic age was 72.4years (InterQuartile Range 61.6-80.2), but there was considerable subtype heterogeneity, particularly among the acute myeloid leukaemias (AML) where medians ranged from 20.3 (IQR 13.9-43.8) for AML 11q23 through to 73.7 (IQR 57.3-79.1) for AML with no recurrent genetic changes. Five-year Relative Survival (RS) estimates varied hugely; from <5% for aggressive entities like therapy-related AML (2.6%, 95% Confidence Interval 0.4-9.0) to >85% for indolent/treatable conditions like chronic myeloid leukaemia (89.8%, 95% CI 84.0-93.6). With a couple of notable exceptions, males experienced higher rates and worse survival than females: the age-standardized incidence rates of several conditions was 2-4 higher in males than females, and the 5-year RS for all subtypes combined was 48.8% (95% CI 46.5-51.2) and 60.4% (95% CI 57.7-62.9) for males and females respectively. During follow-up (potential minimum 2 years and maximum 11years) myelodysplastic syndrome (MDS) progression to AML ranged from 25% for refractory anaemia with excess blasts through to 5% for refractory anaemia with ring sideroblasts: the median interval between MDS and AML diagnosis was 9.0 months (IQR 4.8-17.4months).
The marked incidence and outcome variations seen by subtype, sex and age, confirm the requirement for "real-world" longitudinal data to inform aetiological hypotheses, healthcare planning, and future monitoring of therapeutic change. Several challenges for routine cancer registration were identified, including the need to link more effectively to diagnostic and clinical data sources, and to review policies on the recording of progressions and transformations.
为了为临床实践和研究提供信息,需要基于人群的癌症发病率、患病率和结局信息;但目前缺乏许多髓系恶性肿瘤亚型的当代数据。
在一个具有社会人口代表性的英国约 400 万人口中,髓系恶性肿瘤数据(N=5231 例诊断)来自一个已建立的患者队列。为 20 多种以上的亚型提供了发病率、生存(相对和总体)、转化/进展和患病率信息。
中位诊断年龄为 72.4 岁(四分位距 61.6-80.2),但存在很大的亚型异质性,尤其是急性髓系白血病(AML),其中中位数范围从 AML 11q23 的 20.3(IQR 13.9-43.8)到无复发性遗传改变的 AML 73.7(IQR 57.3-79.1)。五年相对生存率(RS)估计差异很大;从侵袭性实体如治疗相关 AML 的<5%(2.6%,95%置信区间 0.4-9.0)到惰性/可治疗疾病如慢性髓系白血病的>85%(89.8%,95%CI 84.0-93.6)。除了一些值得注意的例外,男性的发病率和生存率均高于女性:几种疾病的年龄标准化发病率男性比女性高 2-4 倍,所有亚型的 5 年 RS 分别为男性 48.8%(95%CI 46.5-51.2)和女性 60.4%(95%CI 57.7-62.9)。在随访期间(潜在最小 2 年,最大 11 年),骨髓增生异常综合征(MDS)向 AML 的进展范围从难治性贫血伴过多原始细胞的 25%到难治性贫血伴环形铁幼粒细胞的 5%:MDS 和 AML 诊断之间的中位间隔为 9.0 个月(四分位距 4.8-17.4 个月)。
通过亚型、性别和年龄观察到的发病率和结局的显著差异,证实了需要“真实世界”的纵向数据来验证病因假说、医疗规划以及未来治疗变化的监测。确定了常规癌症登记面临的一些挑战,包括需要更有效地链接到诊断和临床数据源,并审查关于进展和转化记录的政策。