Emergency Medical Services, Helsinki University Hospital, Helsinki, Finland
Department of Neurology and Clinical Neurosciences, Helsinki University Hospital, Helsinki, Finland.
J Am Heart Assoc. 2016 May 2;5(5):e002808. doi: 10.1161/JAHA.115.002808.
Few studies have discussed the emergency call and prehospital care as a continuous process to decrease the prehospital and in-hospital delays for acute stroke. To identify features associated with early hospital arrival (<90 minutes) and treatment (<120 minutes), we analyzed the operation of current dispatch protocol and emergency medical services and compared stroke recognition by dispatchers and ambulance crews.
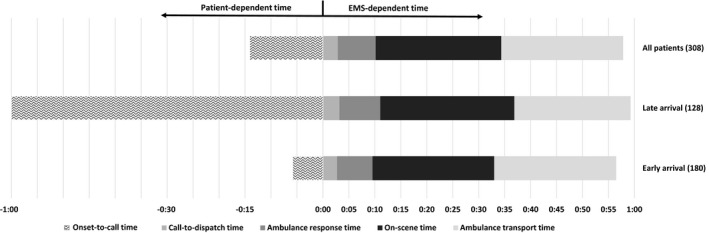
This was a 2-year prospective observational study. All stroke patients who were transported to the hospital by emergency medical services and received recanalization therapy were recruited for the study. For a sample of 308 patients, the stroke code was activated in 206 (67%) and high priority was used in 258 (84%) of the emergency calls. Emergency medical services transported 285 (93%) of the patients using the stroke code and 269 (87%) using high priority. In the univariate analysis, the most dominant predictors of early hospital arrival were transport using stroke code (P=0.001) and high priority (P=0.002) and onset-to-call (P<0.0001) and on-scene times (P=0.052). In the regression analysis, the influences of high-priority transport (P<0.01) and onset-to-call time (P<0.001) prevailed as significant in both dichotomies of early arrival and treatment. The on-scene time was found to be surprisingly long (>23.5 minutes) for both early and late-arriving patients.
Fast emergency medical services activation and ambulance transport promoted early hospital arrival and treatment. Although patient-dependent delays still dominate the prehospital process, it should be ensured that the minutes on the scene are well spent.
很少有研究讨论将紧急呼叫和院前急救作为一个连续的过程,以减少急性脑卒中的院前和院内延误。为了确定与早期医院到达(<90 分钟)和治疗(<120 分钟)相关的特征,我们分析了当前调度协议和紧急医疗服务的运作情况,并比较了调度员和救护人员对脑卒中的识别。
这是一项为期 2 年的前瞻性观察研究。所有通过紧急医疗服务送往医院并接受再通治疗的脑卒中患者均被纳入研究。在 308 名患者的样本中,206 名(67%)患者的脑卒中代码被激活,258 名(84%)患者的紧急电话被列为高优先级。285 名(93%)患者使用脑卒中代码,269 名(87%)患者使用高优先级由紧急医疗服务运送。在单因素分析中,早期到达医院的最主要预测因素是使用脑卒中代码(P=0.001)和高优先级(P=0.002)以及发病到呼叫时间(P<0.0001)和现场时间(P=0.052)。在回归分析中,高优先级转运(P<0.01)和发病到呼叫时间(P<0.001)的影响在早期和晚期到达的两个二分法中都被证明是显著的。令人惊讶的是,现场时间对于早期和晚期到达的患者都很长(>23.5 分钟)。
快速的紧急医疗服务激活和救护车转运促进了早期的医院到达和治疗。尽管患者依赖的延误仍然主导着院前过程,但应确保现场的时间得到充分利用。