Cosgrove Catherine A, Lacey Charles J, Cope Alethea V, Bartolf Angela, Morris Georgina, Yan Celine, Baden Susan, Cole Tom, Carter Darrick, Brodnicki Elizabeth, Shen Xiaoying, Joseph Sarah, DeRosa Stephen C, Peng Lili, Yu Xuesong, Ferrari Guido, Seaman Mike, Montefiori David C, Frahm Nicole, Tomaras Georgia D, Stöhr Wolfgang, McCormack Sheena, Shattock Robin J
Centre for Infection, St George's, University of London, London, United Kingdom.
Hull York Medical School & Centre for Immunology and Infection, University of York, York, United Kingdom.
PLoS One. 2016 May 9;11(5):e0152038. doi: 10.1371/journal.pone.0152038. eCollection 2016.
Defining optimal routes for induction of mucosal immunity represents an important research priority for the HIV-1 vaccine field. In particular, it remains unclear whether mucosal routes of immunization can improve mucosal immune responses.
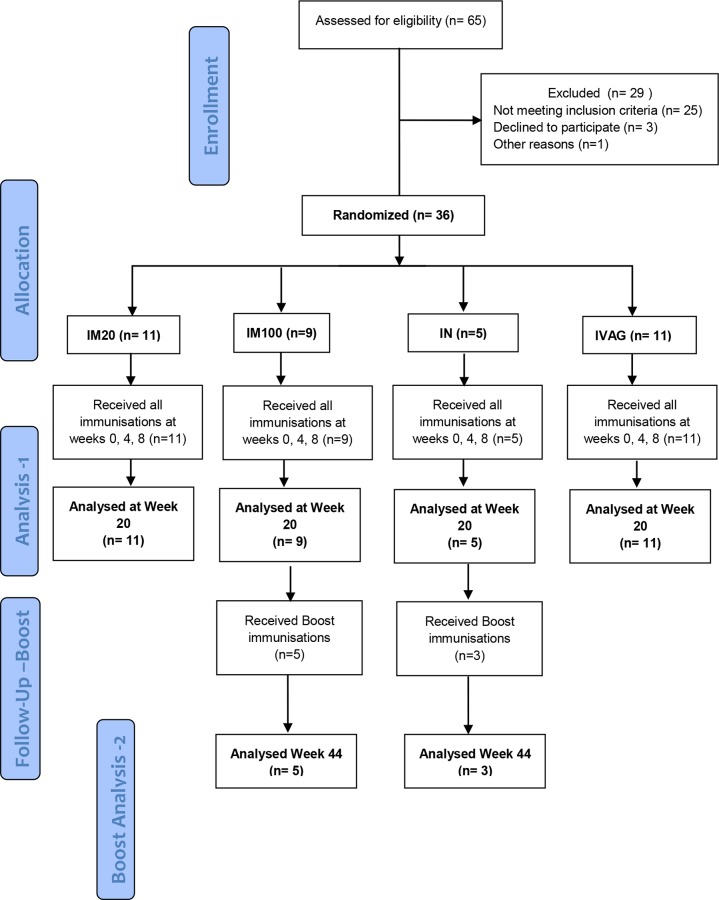
In this randomized two center phase I clinical trial we evaluated the systemic and mucosal immune response to a candidate HIV-1 Clade C CN54gp140 envelope glycoprotein vaccine administered by intramuscular (IM), intranasal (IN) and intravaginal (IVAG) routes of administration in HIV negative female volunteers. IM immunizations were co-administered with Glucopyranosyl Lipid Adjuvant (GLA), IN immunizations with 0.5% chitosan and IVAG immunizations were administered in an aqueous gel.
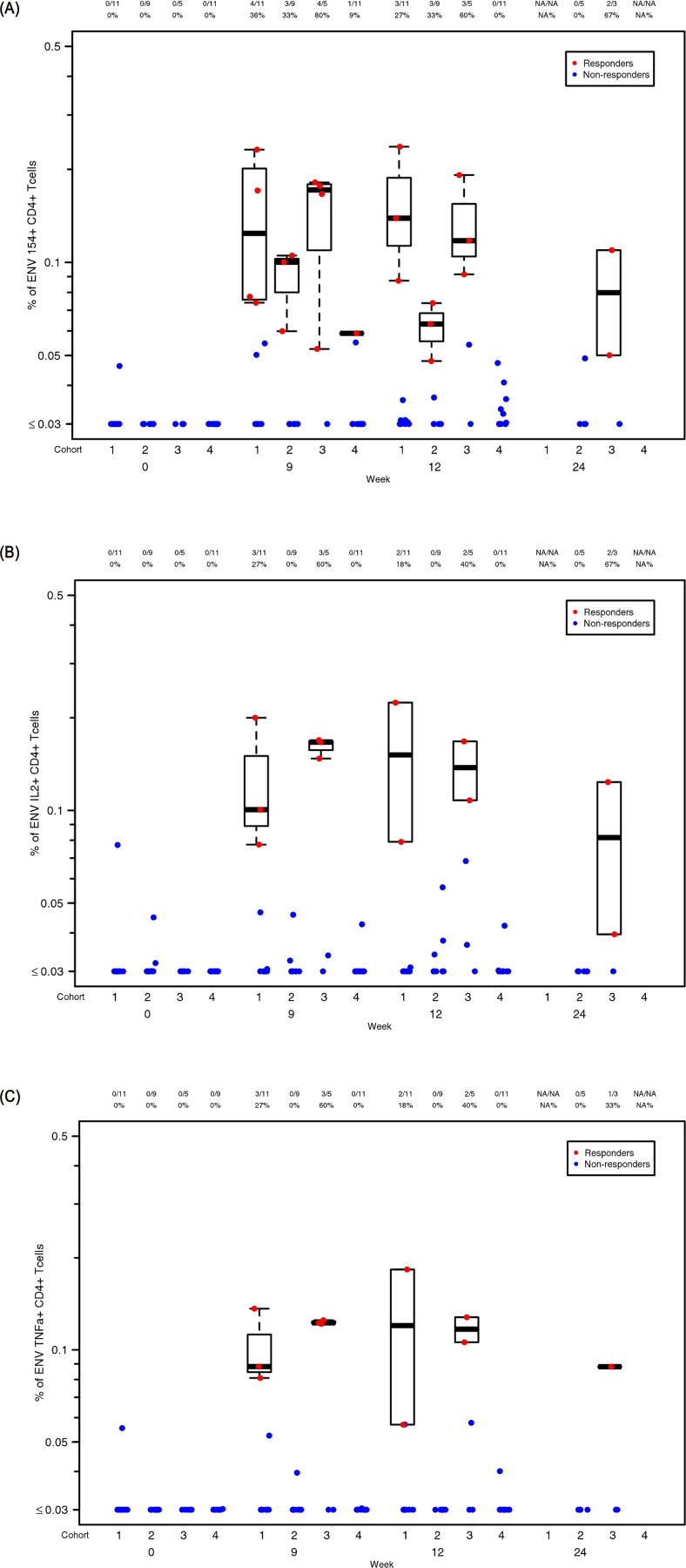
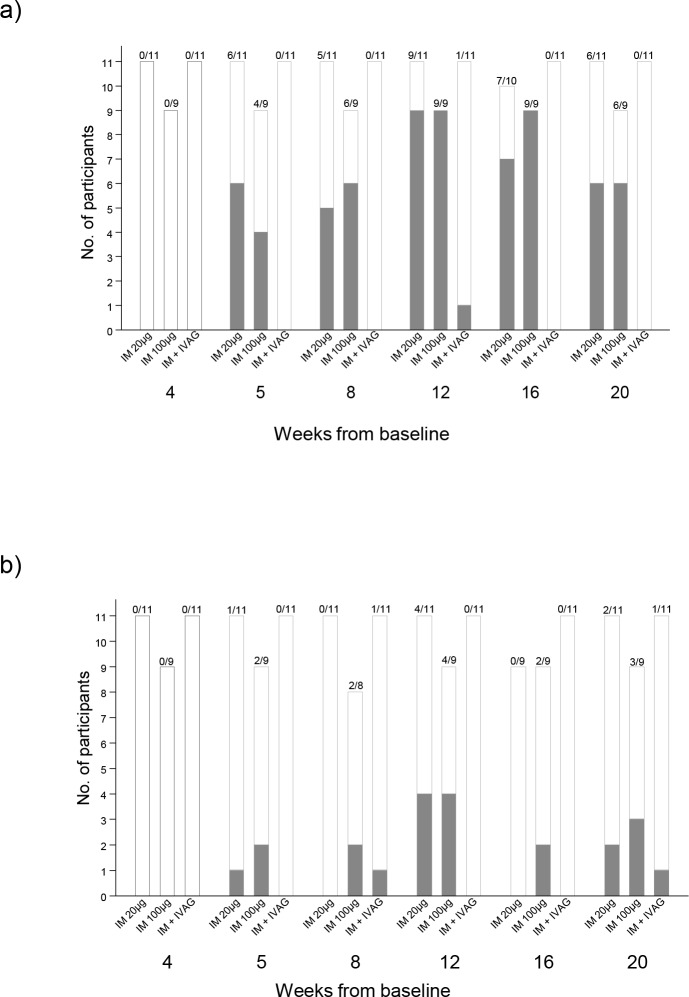
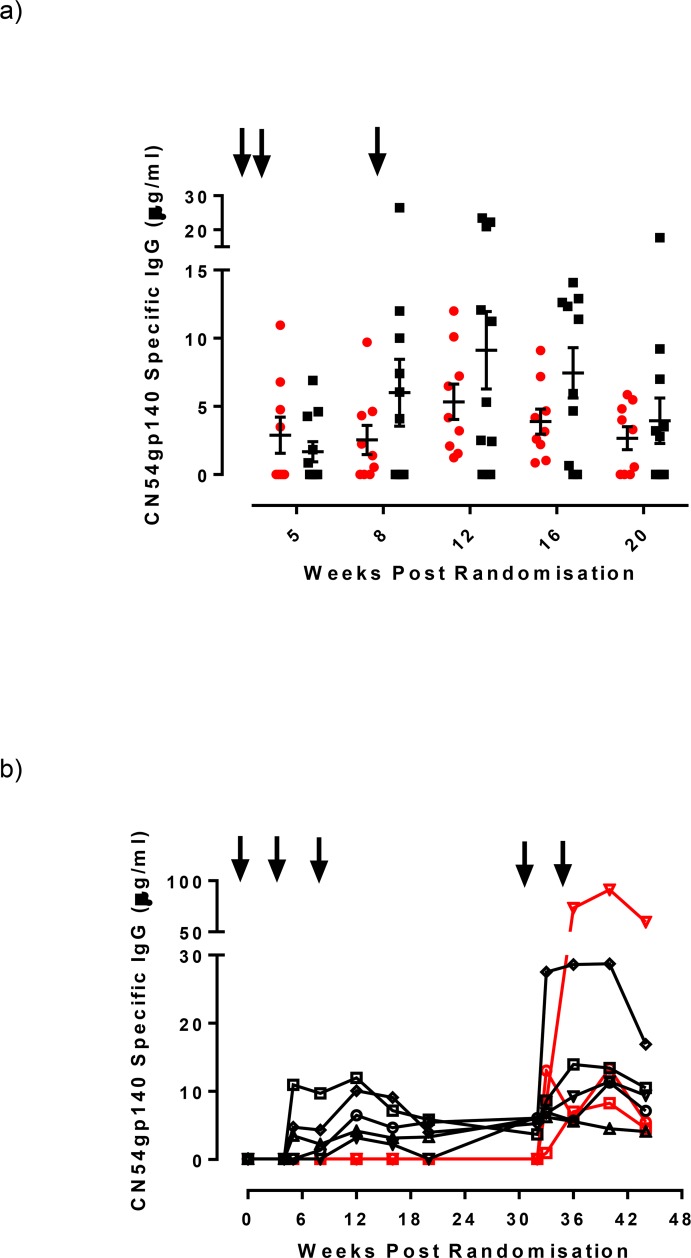
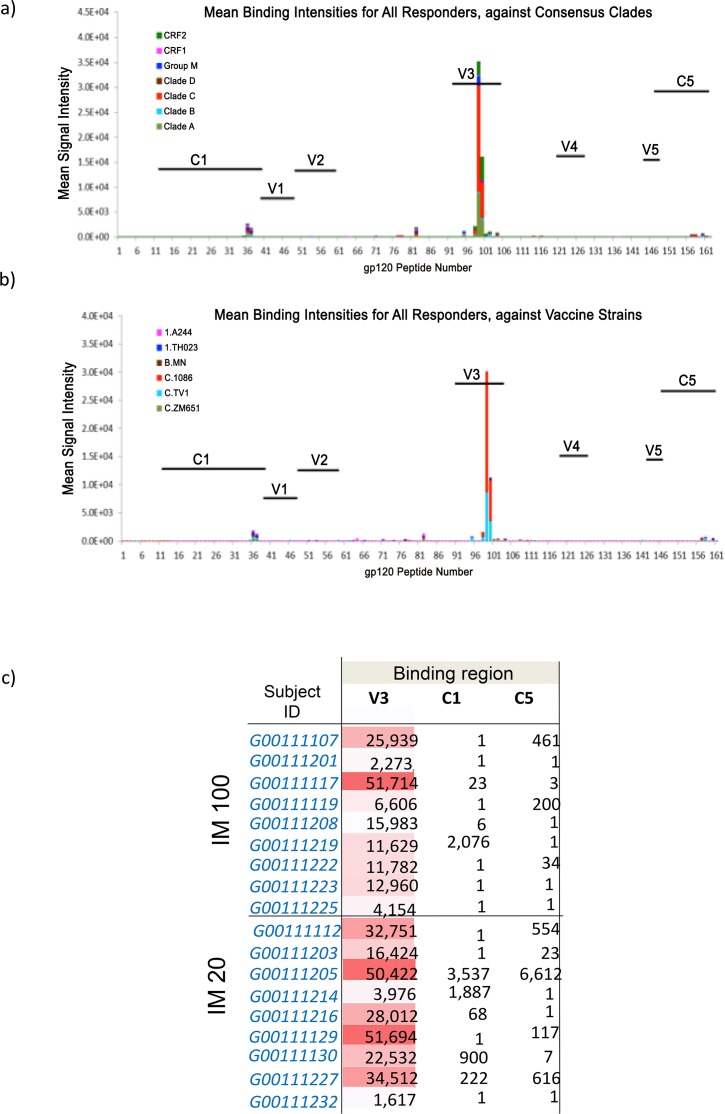
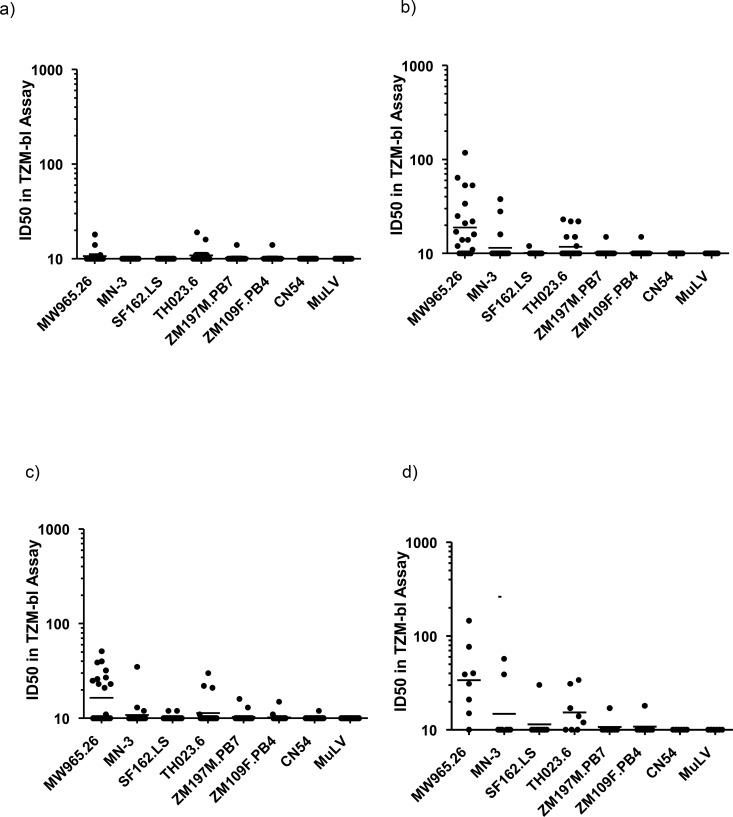
Three IM immunizations of CN54 gp140 at either 20 or 100 μg elicited significantly greater systemic and mucosal antibodies than either IN or IVAG immunizations. Following additional intramuscular boosting we observed an anamnestic antibody response in nasally primed subjects. Modest neutralizing responses were detected against closely matched tier 1 clade C virus in the IM groups. Interestingly, the strongest CD4 T-cell responses were detected after IN and not IM immunization.
These data show that parenteral immunization elicits systemic and mucosal antibodies in women. Interestingly IN immunization was an effective prime for IM boost, while IVAG administration had no detectable impact on systemic or mucosal responses despite IM priming.
EudraCT 2010-019103-27 and the UK Clinical Research Network (UKCRN) Number 11679.
确定诱导黏膜免疫的最佳途径是HIV-1疫苗领域的一项重要研究重点。特别是,黏膜免疫途径是否能改善黏膜免疫反应仍不清楚。
在这项随机双中心I期临床试验中,我们评估了HIV阴性女性志愿者通过肌肉注射(IM)、鼻内(IN)和阴道内(IVAG)途径接种候选HIV-1 C亚型CN54gp140包膜糖蛋白疫苗后的全身和黏膜免疫反应。IM免疫联合吡喃葡萄糖基脂质佐剂(GLA),IN免疫联合0.5%壳聚糖,IVAG免疫采用水凝胶制剂。
20μg或100μg的CN54 gp140进行三次IM免疫诱导产生的全身和黏膜抗体显著多于IN或IVAG免疫。在额外的肌肉注射加强免疫后,我们观察到鼻内初免受试者出现了回忆性抗体反应。在IM组中检测到针对密切匹配的1级C亚型病毒的适度中和反应。有趣的是,最强的CD4 T细胞反应是在IN免疫后而非IM免疫后检测到的。
这些数据表明,胃肠外免疫可在女性中诱导全身和黏膜抗体。有趣的是,IN免疫是IM加强免疫的有效初免方式,而尽管有IM初免,IVAG接种对全身或黏膜反应没有可检测到的影响。
EudraCT 2010-019103-27和英国临床研究网络(UKCRN)编号11679。