Mouton Johannes P, Njuguna Christine, Kramer Nicole, Stewart Annemie, Mehta Ushma, Blockman Marc, Fortuin-De Smidt Melony, De Waal Reneé, Parrish Andy G, Wilson Douglas P K, Igumbor Ehimario U, Aynalem Getahun, Dheda Mukesh, Maartens Gary, Cohen Karen
From the Department of Medicine, Division of Clinical Pharmacology, University of Cape Town, Cape Town (JPM, CN, NK, AS, UM, MB, MFDS, RDW, GM, KC); Department of Medicine, East London Hospital Complex and Walter Sisulu University, East London (AGP); Department of Medicine, Edendale Hospital, Pietermaritzburg, South Africa (DPKW), US Centers for Disease Control and Prevention, Pretoria (EUI, GA); National Department of Health, Pretoria (MD); and Pharmaceutical Services, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa (MD).
Medicine (Baltimore). 2016 May;95(19):e3437. doi: 10.1097/MD.0000000000003437.
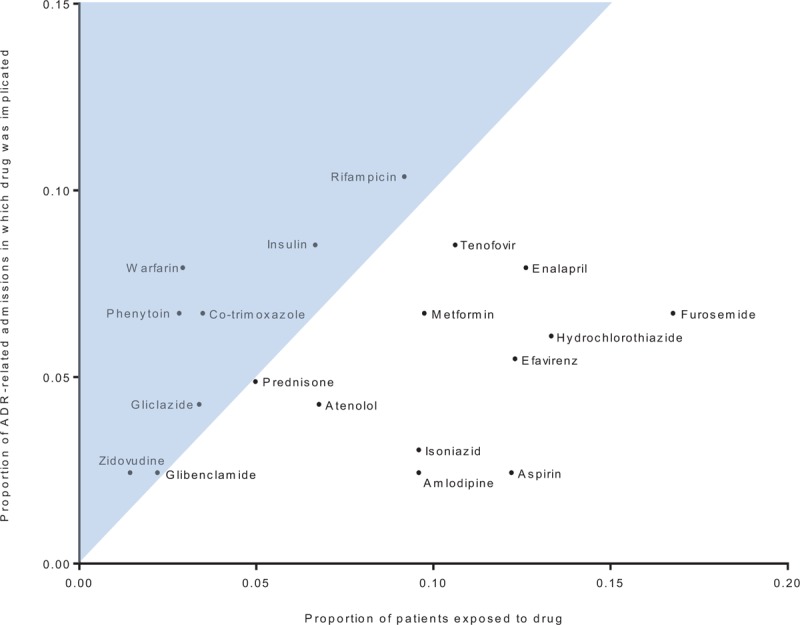
Limited data exist on the burden of serious adverse drug reactions (ADRs) in sub-Saharan Africa, which has high HIV and tuberculosis prevalence. We determined the proportion of adult admissions attributable to ADRs at 4 hospitals in South Africa. We characterized drugs implicated in, risk factors for, and the preventability of ADR-related admissions.We prospectively followed patients admitted to 4 hospitals' medical wards over sequential 30-day periods in 2013 and identified suspected ADRs with the aid of a trigger tool. A multidisciplinary team performed causality, preventability, and severity assessment using published criteria. We categorized an admission as ADR-related if the ADR was the primary reason for admission.There were 1951 admissions involving 1904 patients: median age was 50 years (interquartile range 34-65), 1057 of 1904 (56%) were female, 559 of 1904 (29%) were HIV-infected, and 183 of 1904 (10%) were on antituberculosis therapy (ATT). There were 164 of 1951 (8.4%) ADR-related admissions. After adjustment for age and ATT, ADR-related admission was independently associated (P ≤ 0.02) with female sex (adjusted odds ratio [aOR] 1.51, 95% confidence interval [95% CI] 1.06-2.14), increasing drug count (aOR 1.14 per additional drug, 95% CI 1.09-1.20), increasing comorbidity score (aOR 1.23 per additional point, 95% CI 1.07-1.41), and use of antiretroviral therapy (ART) if HIV-infected (aOR 1.92 compared with HIV-negative/unknown, 95% CI 1.17-3.14). The most common ADRs were renal impairment, hypoglycemia, liver injury, and hemorrhage. Tenofovir disoproxil fumarate, insulin, rifampicin, and warfarin were most commonly implicated, respectively, in these 4 ADRs. ART, ATT, and/or co-trimoxazole were implicated in 56 of 164 (34%) ADR-related admissions. Seventy-three of 164 (45%) ADRs were assessed as preventable.In our survey, approximately 1 in 12 admissions was because of an ADR. The range of ADRs and implicated drugs reflect South Africa's high HIV and tuberculosis burden. Identification and management of these ADRs should be considered in HIV and tuberculosis care and treatment programs and should be emphasized in health care worker training programmes.
关于撒哈拉以南非洲地区严重药物不良反应(ADR)负担的数据有限,该地区艾滋病毒和结核病的患病率很高。我们确定了南非4家医院因ADR导致的成人住院比例。我们对与ADR相关的住院所涉及的药物、危险因素及可预防性进行了描述。2013年,我们对4家医院内科病房连续30天入院的患者进行了前瞻性跟踪,并借助触发工具识别疑似ADR。一个多学科团队使用已发表的标准进行因果关系、可预防性和严重程度评估。如果ADR是入院的主要原因,我们将此次住院归类为与ADR相关。
共有1951例住院病例,涉及1904名患者:年龄中位数为50岁(四分位间距34 - 65岁),1904名患者中有1057名(56%)为女性,1904名患者中有559名(29%)感染艾滋病毒,1904名患者中有183名(10%)正在接受抗结核治疗(ATT)。1951例中有164例(8.4%)与ADR相关的住院。在对年龄和ATT进行调整后,与ADR相关的住院独立相关(P≤0.02)于女性(调整后的优势比[aOR]为1.51,95%置信区间[95%CI]为1.06 - 2.14)、药物数量增加(每增加一种药物aOR为1.14,95%CI为1.09 - 1.20)、合并症评分增加(每增加一分aOR为1.23,95%CI为1.07 - 1.41)以及感染艾滋病毒时使用抗逆转录病毒疗法(ART)(与艾滋病毒阴性/未知相比aOR为1.92,95%CI为1.17 - 3.14)。最常见的ADR是肾功能损害、低血糖、肝损伤和出血。替诺福韦酯、胰岛素、利福平和华法林分别最常与这4种ADR相关。ART、ATT和/或复方新诺明涉及164例与ADR相关住院中的56例(34%)。164例中有73例(45%)ADR被评估为可预防。
在我们的调查中,约每12例住院中有1例是由ADR导致。ADR的范围和涉及的药物反映了南非艾滋病毒和结核病的高负担。在艾滋病毒和结核病护理及治疗项目中应考虑识别和管理这些ADR,并应在医护人员培训项目中予以强调。