Carneiro Arie, Sakuramoto Paulo, Wroclawski Marcelo Langer, Forseto Pedro Herminio, Den Julio Alexandre, Bautzer Carlos Ricardo Doi, Lins Leonardo Monte Marques, Kataguiri Andre, Yamada Fernanda Batistini, Teixeira Gabriel Kushiyama, Tobias-Machado Marcos, Pompeo Antonio Carlos Lima
Hospital Israelita Albert Einstein, SP, Brasil.
Departamento de Urologia, Faculdade de Medicina do ABC, São Paulo, Brasil.
Int Braz J Urol. 2016 Mar-Apr;42(2):284-92. doi: 10.1590/S1677-5538.IBJU.2014.0517.
This study compared the suprapubic (SP) versus retropubic (RP) prostatectomy for the treatment of large prostates and evaluated perioperative surgical morbidity and improvement of urinary symptoms.
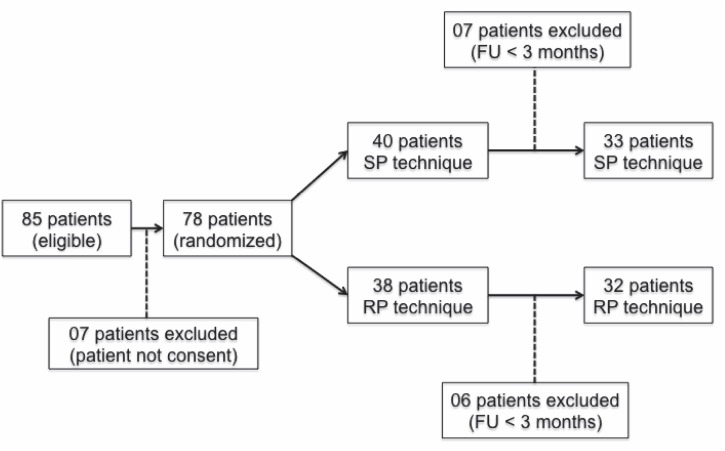
In this single centre, prospective, randomised study, 65 consecutive patients with LUTS and surgical indication with prostate volume greater than 75g underwent open prostatectomy to compare the RP (32 patients) versus SP (33 patients) technique.
The SP group exhibited a higher incidence of complications (p=0.002). Regarding voiding pattern analysis (IPSS and flowmetry), both were significantly effective compared to pre-treatment baseline. The RP group parameters were significantly better, with higher peak urinary flow (SP: 16.77 versus RP: 23.03mL/s, p=0.008) and a trend of lower IPSS score (SP: 6.67 versus RP 4.14, p=0.06). In a subgroup evaluation of patients with prostate volumes larger than 100g, blood loss was lower in those undergoing SP prostatectomy (p=0.003). Patients with prostates smaller than 100g in the SP group exhibited a higher incidence of low grade late complications (p=0.004).
The SP technique was related to a higher incidence of minor complications in the late postoperative period. High volume prostates were associated with increased bleeding when the RP technique was utilized. The RP prostatectomy was associated with higher peak urinary flow and a trend of a lower IPSS Score.
本研究比较耻骨上(SP)与耻骨后(RP)前列腺切除术治疗大体积前列腺的效果,并评估围手术期手术并发症及尿路症状的改善情况。
在这项单中心、前瞻性、随机研究中,65例连续的有下尿路症状且手术指征为前列腺体积大于75g的患者接受了开放性前列腺切除术,以比较RP(32例患者)与SP(33例患者)技术。
SP组并发症发生率较高(p = 0.002)。关于排尿模式分析(国际前列腺症状评分[IPSS]和尿流率测定),与治疗前基线相比两者均显著有效。RP组参数明显更好,尿流峰值更高(SP:16.77 对比 RP:23.03mL/s,p = 0.008),且IPSS评分有降低趋势(SP:6.67 对比 RP 4.14,p = 0.06)。在前列腺体积大于100g的患者亚组评估中,接受SP前列腺切除术的患者失血量更低(p = 0.003)。SP组中前列腺小于100g的患者低度晚期并发症发生率较高(p = 0.004)。
SP技术与术后晚期轻微并发症发生率较高有关。使用RP技术时,大体积前列腺与出血增加相关。RP前列腺切除术与更高的尿流峰值及IPSS评分降低趋势相关。