Marvin Michael R, Inzucchi Silvio E, Besterman Brian J
1 Pronia Medical Systems, LLC , Louisville, Kentucky.
2 Section of Endocrinology, Yale University School of Medicine , New Haven, Connecticut.
Diabetes Technol Ther. 2016 Aug;18(8):480-6. doi: 10.1089/dia.2016.0101. Epub 2016 Jun 3.
The management of hyperglycemia in the intensive care unit has been a controversial topic for more than a decade, with target ranges varying from 80-110 mg/dL to <200 mg/dL. Multiple insulin infusion protocols exist, including several computerized protocols, which have attempted to achieve these targets. Importantly, compliance with these protocols has not been a focus of clinical studies.
GlucoCare™, a Food and Drug Administration (FDA)-cleared insulin-dosing calculator, was originally designed based on the Yale Insulin Infusion Protocol to target 100-140 mg/dL and has undergone several modifications to reduce hypoglycemia. The original Yale protocol was modified from 100-140 mg/dL to a range of 120-140 mg/dL (GlucoCare 120-140) and then to 140 mg/dL (GlucoCare 140, not a range but a single blood glucose [BG] level target) in an iterative and evidence-based manner to eliminate hypoglycemia <70 mg/dL. The final modification [GlucoCare 140(B)] includes the addition of bolus insulin "midprotocol" during an insulin infusion to reduce peak insulin rates for insulin-resistant patients. This study examined the results of these protocol modifications and evaluated the role of compliance with the protocol in the incidence of hypoglycemia <70 mg/dL.
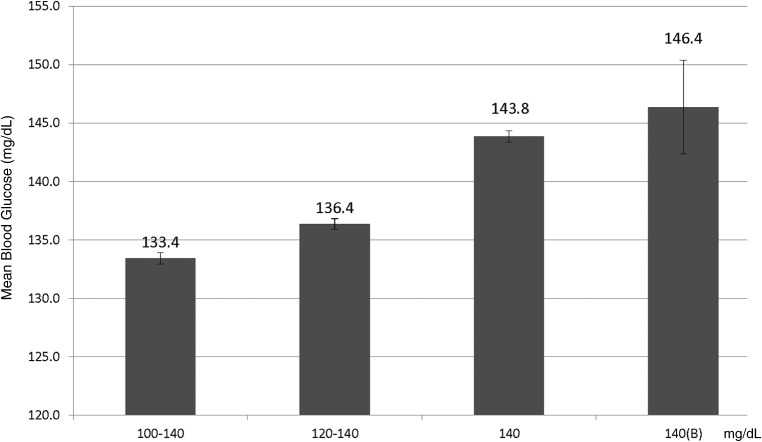
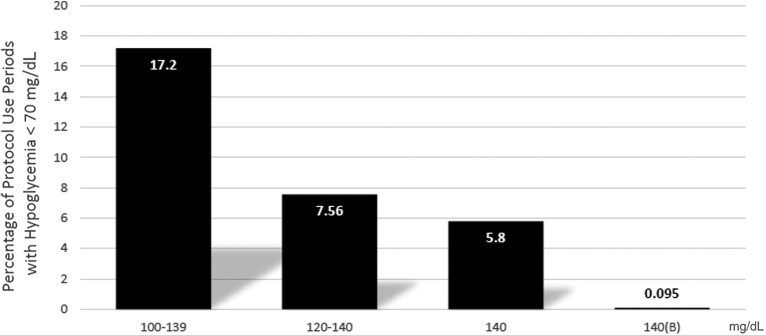
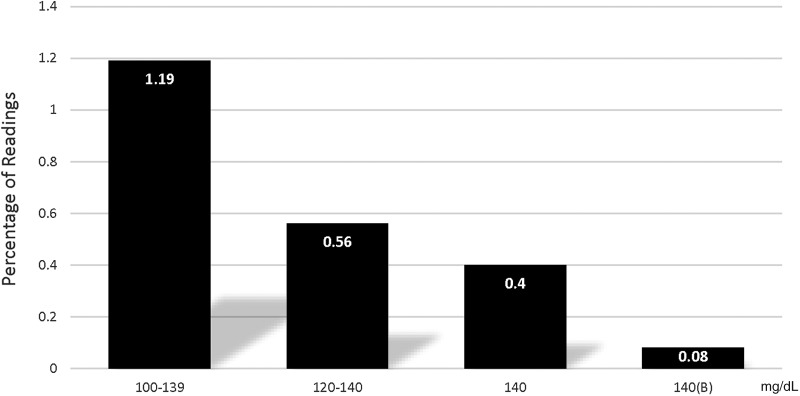
Protocol modifications resulted in mean BG levels of 133.4, 136.4, 143.8, and 146.4 mg/dL and hypoglycemic BG readings <70 mg/dL of 0.998%, 0.367%, 0.256%, and 0.04% for the 100-140, 120-140, 140, and 140(B) protocols, respectively (P < 0.001). Adherence to the glucose check interval significantly reduced the incidence of hypoglycemia (P < 0.001). Protocol modifications led to a reduction in peak insulin infusion rates (P < 0.001) and the need for dextrose-containing boluses (P < 0.001).
This study demonstrates that refinements in protocol design can improve glucose control in critically ill patients and that the use of GlucoCare 140(B) can eliminate all significant hypoglycemia while achieving mean glucose levels between 140 and 150 mg/dL. In addition, attention to the timely performance of glucose levels can also reduce hypoglycemic events.
十多年来,重症监护病房高血糖的管理一直是一个有争议的话题,目标范围从80 - 110毫克/分升到<200毫克/分升不等。存在多种胰岛素输注方案,包括几种计算机化方案,这些方案试图实现这些目标。重要的是,对这些方案的依从性并非临床研究的重点。
GlucoCare™是一种经美国食品药品监督管理局(FDA)批准的胰岛素剂量计算器,最初基于耶鲁胰岛素输注方案设计,目标是100 - 140毫克/分升,并经过多次修改以降低低血糖发生率。最初的耶鲁方案从100 - 140毫克/分升修改为120 - 140毫克/分升范围(GlucoCare 120 - 140),然后以迭代和循证的方式修改为140毫克/分升(GlucoCare 140,不是一个范围而是单个血糖[BG]水平目标),以消除<70毫克/分升的低血糖。最终修改版[GlucoCare 140(B)]包括在胰岛素输注期间添加推注胰岛素“方案中期”,以降低胰岛素抵抗患者的胰岛素峰值速率。本研究检查了这些方案修改的结果,并评估了对方案的依从性在<70毫克/分升低血糖发生率中的作用。
方案修改导致100 - \alpha40、120 - \alpha40、140和140(B)方案的平均BG水平分别为133.4、136.4、143.8和146.4毫克/分升,低血糖BG读数<70毫克/分升的发生率分别为0.998%、0.367%、0.256%和0.04%(P < 0.001)。坚持血糖检查间隔可显著降低低血糖发生率(P < 0.001)。方案修改导致胰岛素输注峰值速率降低(P < 0.001)以及对含葡萄糖推注的需求降低(P < 0.001)。
本研究表明,方案设计的改进可改善危重症患者的血糖控制,使用GlucoCare 140(B)可消除所有显著低血糖情况,同时实现平均血糖水平在140至150毫克/分升之间。此外,关注血糖水平的及时检测也可减少低血糖事件。