Reddy Dereddi Raja Shekar, Singh Tarun D, Guru Pramod K, Sakusic Amra, Gajic Ognjen, O'Horo John C, Rabinstein Alejandro A
Department of Medicine, Division of Pulmonary and Critical Care Medicine, Mayo Clinic, Rochester, MN; Department of Medicine, Multidisciplinary Epidemiology and Translational Research in Intensive Care, Emergency and Perioperative Medicine (METRIC), Mayo Clinic, Rochester, MN.
Department of Medicine, Multidisciplinary Epidemiology and Translational Research in Intensive Care, Emergency and Perioperative Medicine (METRIC), Mayo Clinic, Rochester, MN; Department of Neurology, Division of Critical Care Neurology, Mayo Clinic, Rochester, MN.
J Crit Care. 2016 Aug;34:12-6. doi: 10.1016/j.jcrc.2016.03.008. Epub 2016 Mar 16.
Up to 80% of critically ill patients have acute neurologic dysfunction syndromes. We evaluated interrater reliability between the examination by the investigator and the charted assessment by the nurse because the accuracy and reliability of detailed data sets extracted from the electronic medical records represents a keystone for creating EMR-based definitions.
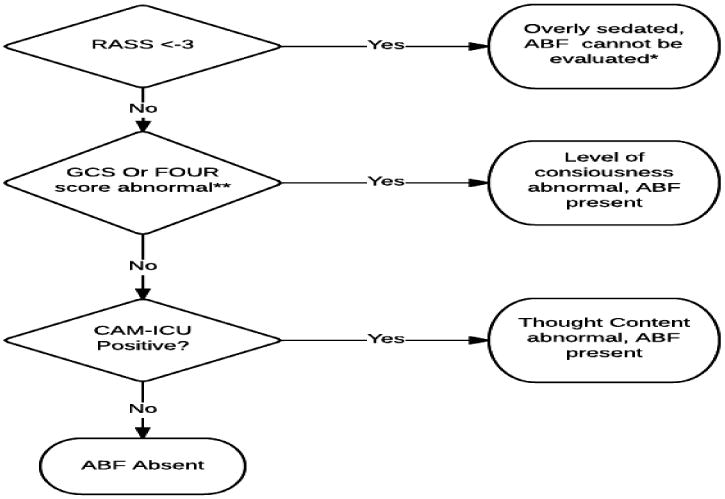
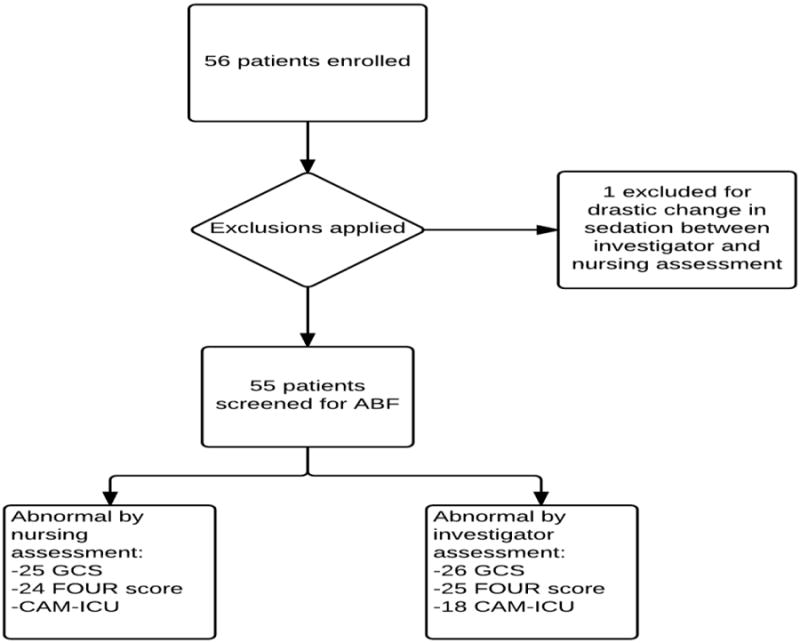
We conducted a prospective observational study of intensive care unit (ICU) patients to assess the reliability of charted Confusion Assessment Method for the ICU, Glasgow Coma Scale (GSC), Full Outline of Unresponsiveness, and Richmond Agitation Sedation Scale (RASS) scores, and a composite measure of ABF defined as new-onset coma or delirium. Trained investigator blinded to nursing assessments performed the neurologic evaluations that were compared with nursing documentation.
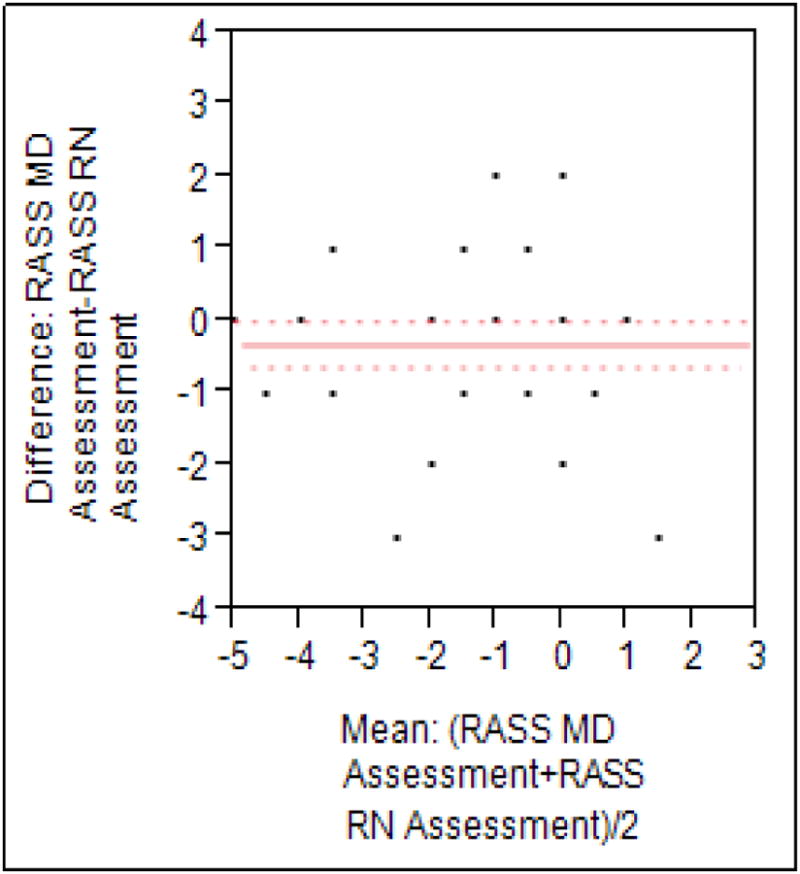
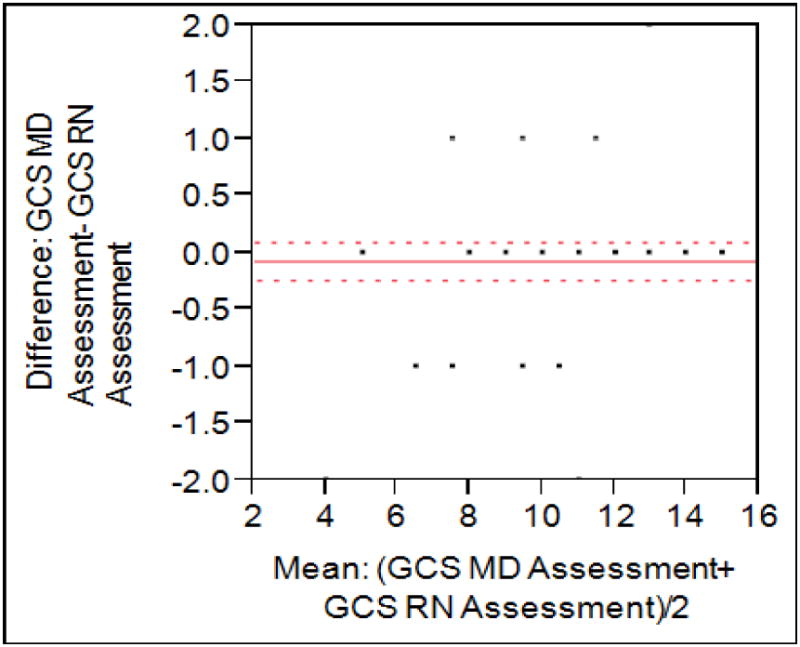
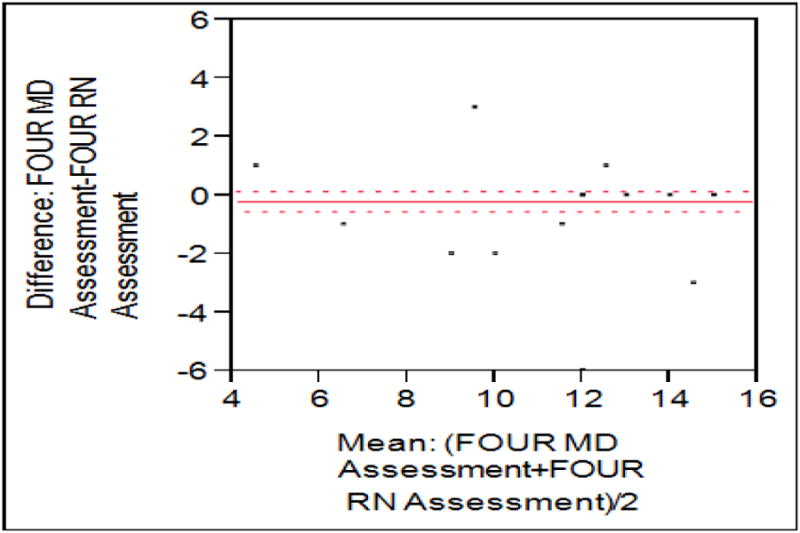
A total of 202 observations were performed in 55 ICU patients. Excellent correlation was noted for GCS and Full Outline of Unresponsiveness scores on Bland-Altman plots (Pearson correlation 0.87 and 0.92, respectively). Correlation for Confusion Assessment Method for the ICU was also high (κ= 0.86; 95% confidence interval [CI], 0.70-1.01). Richmond Agitation Sedation Scale had good agreement when scores were dichotomized as oversedated (less than -2) vs not oversedated, with κ= 0.76 (95% CI, 0.54-0.98). Investigator assessment and nurse charting were highly concordant (κ= 0.84; 95% CI, 0.71-0.99).
Neurologic assessments documented on the EMR are reliable.
高达80%的重症患者患有急性神经功能障碍综合征。我们评估了研究者检查与护士记录评估之间的评分者间可靠性,因为从电子病历中提取的详细数据集的准确性和可靠性是创建基于电子病历定义的关键。
我们对重症监护病房(ICU)患者进行了一项前瞻性观察研究,以评估记录的ICU意识模糊评估方法、格拉斯哥昏迷量表(GSC)、无反应性全面概述和里士满躁动镇静量表(RASS)评分的可靠性,以及定义为新发昏迷或谵妄的ABF综合指标。对护理评估不知情的经过培训的研究者进行神经学评估,并与护理记录进行比较。
对55例ICU患者共进行了202次观察。在Bland-Altman图上,GSC和无反应性全面概述评分具有极好的相关性(Pearson相关性分别为0.87和0.92)。ICU意识模糊评估方法的相关性也很高(κ=0.86;95%置信区间[CI],0.70-1.01)。当将RASS评分分为镇静过度(小于-2)与未镇静过度时,一致性良好,κ=0.76(95%CI,0.54-0.98)。研究者评估与护士记录高度一致(κ=0.84;95%CI,0.71-0.99)。
电子病历中记录的神经学评估是可靠的。