Contou Damien, Dorison Matthieu, Rosman Jérémy, Schlemmer Frédéric, Gibelin Aude, Foulet Françoise, Botterel Françoise, Carteaux Guillaume, Razazi Keyvan, Brun-Buisson Christian, Mekontso Dessap Armand, de Prost Nicolas
Groupe Henri Mondor-Albert Chenevier, Centre Hospitalier Universitaire Henri Mondor, DHU A-TVB, Service de Réanimation Médicale, Assistance Publique-Hôpitaux de Paris, 51, Avenue du Maréchal de Lattre de Tassigny, 94010, Créteil Cedex, France.
Groupe de Recherche CARMAS, Faculté de Médecine de Créteil, Université Paris Est Créteil, 94010, Créteil, France.
Ann Intensive Care. 2016 Dec;6(1):52. doi: 10.1186/s13613-016-0156-2. Epub 2016 Jun 13.
The detection of Aspergillus spp. in endotracheal aspirate cultures of mechanically ventilated patients may reflect either colonization or infection. However, little is known about the prevalence and the impact on outcome of respiratory tract sample positive for Aspergillus during the acute respiratory distress syndrome (ARDS).
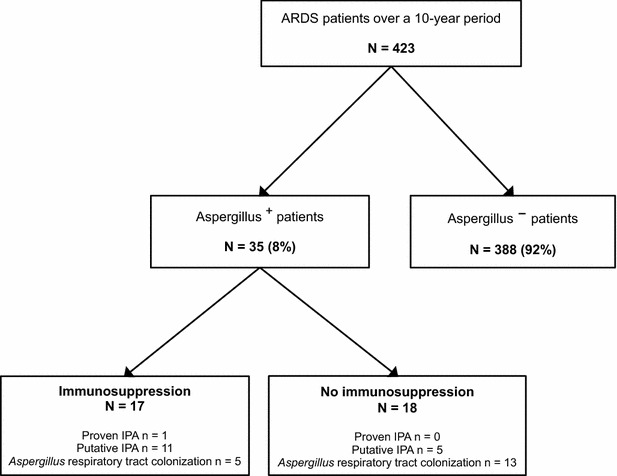
We conducted a monocentric, retrospective study over a 10-year period (January 2006-December 2015) in the ICU of a university hospital. All consecutive adult patients with ARDS were included, and the diagnosis of invasive pulmonary aspergillosis was assessed using a previously validated algorithm.
In total, 423 ARDS patients were included with 35 patients [8.3 %, 95 % CI (5.4-10.6)] having at least one respiratory tract sample positive for Aspergillus (Aspergillus(+) patients) after a median delay of 3 days (1-11) following ICU admission. Comorbidities did not differ between Aspergillus(+) and Aspergillus(-) patients except for more frequent immunosuppression in Aspergillus(+) patients (40 vs. 22 %; p = 0.02). There was no difference between Aspergillus(-) and Aspergillus(+) patients regarding in-ICU mortality, ventilator-free days at day 28, and incidence of ventilator-associated pneumonia, but need for renal replacement therapy was higher in Aspergillus(+) patients than in others (49 vs. 27 %; p = 0.01). Seventeen [4.0 %, 95 % CI (2.1-5.9)] patients had putative/proven aspergillosis. After adjusting on covariates associated with ICU mortality, putative/proven aspergillosis was associated with in-ICU mortality [aOR = 9.58 (1.97-46.52); p = 0.005], while Aspergillus colonization was not [aOR = 0.64 (0.21-1.99); p = 0.44].
Eight percent of ARDS patients had Aspergillus spp.-positive respiratory tract cultures. These had a higher risk of mortality only when categorized as having putative or proven invasive pulmonary aspergillosis.
在机械通气患者的气管内吸出物培养中检测曲霉菌属可能反映定植或感染情况。然而,对于急性呼吸窘迫综合征(ARDS)期间呼吸道样本曲霉菌阳性的患病率及其对预后的影响知之甚少。
我们在一家大学医院的重症监护病房进行了一项为期10年(2006年1月至2015年12月)的单中心回顾性研究。纳入所有连续的成年ARDS患者,并使用先前验证的算法评估侵袭性肺曲霉病的诊断。
总共纳入423例ARDS患者,其中35例[8.3%,95%CI(5.4 - 10.6)]在入住重症监护病房后中位延迟3天(1 - 11天)后至少有一份呼吸道样本曲霉菌阳性(曲霉菌阳性患者)。除曲霉菌阳性患者免疫抑制更频繁外(40%对22%;p = 0.02),曲霉菌阳性和曲霉菌阴性患者的合并症无差异。曲霉菌阴性和曲霉菌阳性患者在重症监护病房死亡率、第28天无呼吸机天数以及呼吸机相关性肺炎发生率方面无差异,但曲霉菌阳性患者肾脏替代治疗的需求高于其他患者(49%对27%;p = 0.01)。17例[4.0%,95%CI(2.1 - 5.9)]患者患有疑似/确诊曲霉菌病。在对与重症监护病房死亡率相关的协变量进行调整后,疑似/确诊曲霉菌病与重症监护病房死亡率相关[aOR = 9.58(1.97 - 46.52);p = 0.005],而曲霉菌定植则不然[aOR = 0.64(0.21 - 1.99);p = 0.44]。
8%的ARDS患者呼吸道培养曲霉菌属阳性。只有当归类为疑似或确诊侵袭性肺曲霉病时,这些患者的死亡风险才更高。