Wang Yue-Shen, Tian Jing, Han Yong, Han Shu-Mei, Shi Sheng-Bin
Department of Oncology, Jilin People's Hospital, Jilin, Jilin, P.R. China.
Oncol Res. 2016;24(2):129-35. doi: 10.3727/096504016X14618564639213.
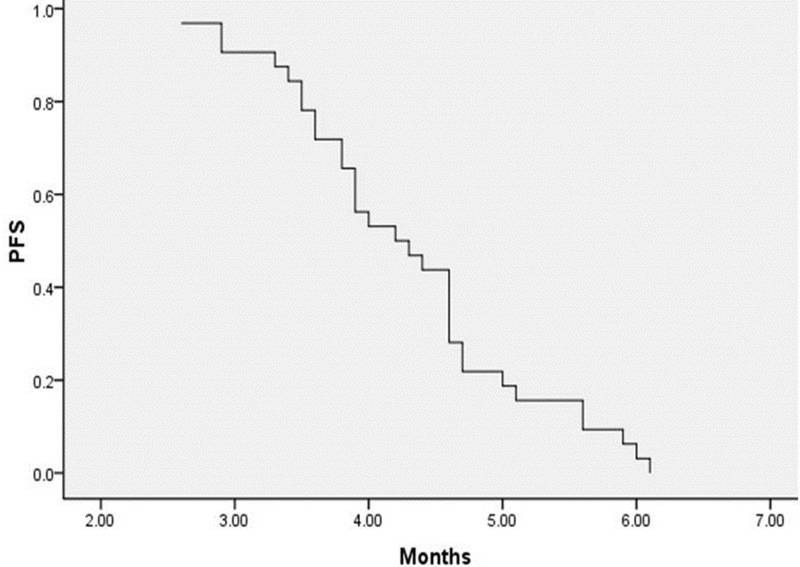
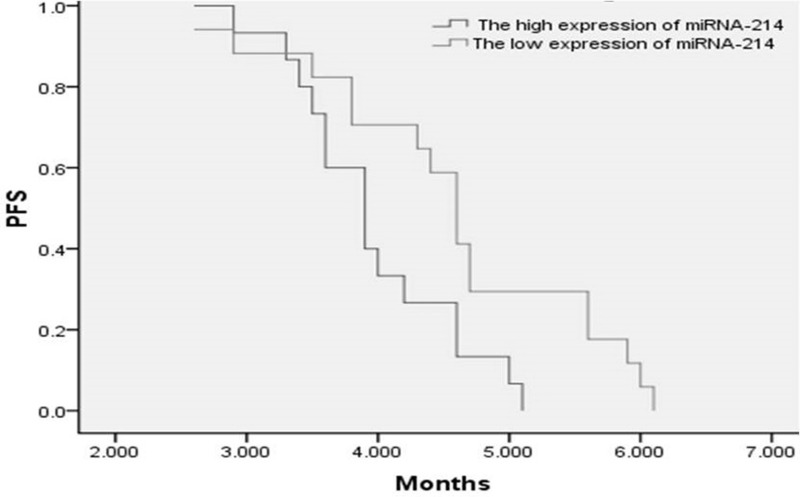
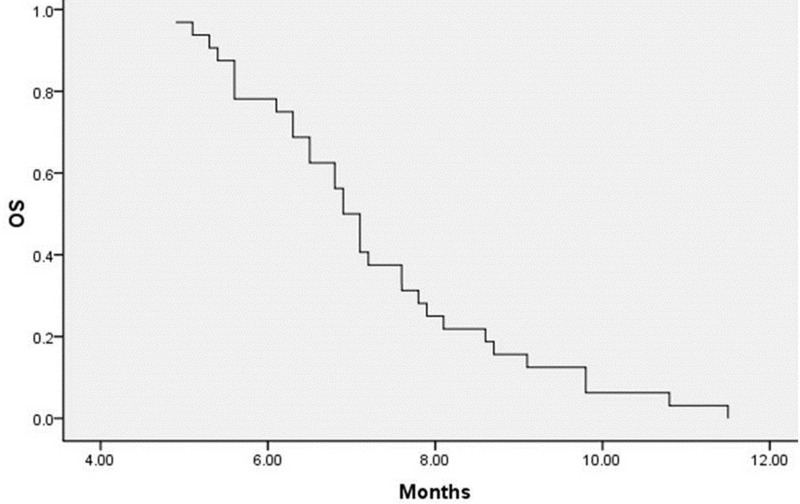
We evaluated the efficacy and feasibility of the combination of gemcitabine plus vinorelbine in patients with platinum-based chemotherapy-refractory esophageal cancer. We enrolled 35 patients who received gemcitabine plus vinorelbine as second-line treatment after platinum-based chemotherapy failure between May 2009 and April 2012. Dosage: gemcitabine 1,000 mg/m(2) plus vinorelbine 25 mg/m(2); all drugs were administered on days 1 and 8 of a 21-day cycle, and this was continued until failure or unacceptable toxicity. A total of 125 cycles of treatment were administered, and all patients received at least two cycles of treatment (two to five cycles; median number of cycles: three). Thirty-two patients were evaluable for response. The response rate was 31.3%, and the disease control rate (partial response plus stable disease) was 62.5%. The progression-free survival (PFS) was 4.3 ± 0.2 months [95% confidence interval (CI), 4.0-4.6], and the median overall survival (OS) was 7.3 ± 0.3 months (95% CI, 6.7-7.8). In the subgroup analysis, median PFS was 4.0 ± 0.2 months (95% CI, 3.6-4.3) in patients with high expression of miRNA-214, while it was 4.6 ± 0.3 months (95% CI, 4.1-5.1) in patients with low expression of miRNA-214 (log rank = 0.023). Myelosuppression with neutropenia and thrombocytopenia was the most common side effect observed with this combination regimen, and higher than grade 3 neutropenia and thrombocytopenia were observed in 10 (31.3%) and 8 patients (25.0%), respectively. Grade 3 fatigue was the most common nonhematologic toxicity, which was observed in 2 (6.1%) patients. The combination of gemcitabine plus vinorelbine was well tolerated as second-line treatment for platinum-based chemotherapy-refractory esophageal cancer patients and appeared to provide enhanced clinical activity especially in patients with low expression of miRNA-214.
我们评估了吉西他滨联合长春瑞滨用于铂类化疗难治性食管癌患者的疗效和可行性。我们纳入了35例在2009年5月至2012年4月期间铂类化疗失败后接受吉西他滨联合长春瑞滨作为二线治疗的患者。剂量:吉西他滨1000mg/m²加长春瑞滨25mg/m²;所有药物在21天周期的第1天和第8天给药,持续至疾病进展或出现不可接受的毒性。共进行了125个周期的治疗,所有患者至少接受了两个周期的治疗(两至五个周期;中位周期数:三个)。32例患者可评估疗效。缓解率为31.3%,疾病控制率(部分缓解加病情稳定)为62.5%。无进展生存期(PFS)为4.3±0.2个月[95%置信区间(CI),4.0 - 4.6],中位总生存期(OS)为7.3±0.3个月(95%CI,6.7 - 7.8)。在亚组分析中,miRNA - 214高表达患者的中位PFS为4.0±0.2个月(95%CI,3.6 - 4.3),而miRNA - 214低表达患者的中位PFS为4.6±0.3个月(95%CI,4.1 - 5.1)(对数秩检验=0.023)。中性粒细胞减少和血小板减少的骨髓抑制是该联合方案最常见的副作用,分别有10例(31.3%)和8例(25.0%)患者出现3级以上中性粒细胞减少和血小板减少。3级疲劳是最常见的非血液学毒性,有2例(6.1%)患者出现。吉西他滨联合长春瑞滨作为铂类化疗难治性食管癌患者的二线治疗耐受性良好,尤其在miRNA - 214低表达患者中似乎具有更强的临床活性。