K Kandhari V, M Desai M, S Bava S, N Wade R
Department of Orthopaedics, Seth G. S. Medical College and K. E. M. Hospital. Mumbai. India.
J Orthop Case Rep. 2015 Oct-Dec;5(4):36-9. doi: 10.13107/jocr.2250-0685.341.
Chances of avascular necrosis of acetabulum are rare as it enjoys a rich blood supply. But cases of post - traumatic avascular necrosis of acetabulum following fracture of posterior column have been well documented. Importance of identifying and suspecting the avascular necrosis of acetabulum is essential in cases of failed fixation of fracture acetabulum, previously operated using extensile approach to acetabulum; either extended anterior ilio - femoral or tri - radiate approach. Such patients usually present with repeated deep bone infection or with early failure of fixation with aseptic loosening and migration of its components. We present a similar case.
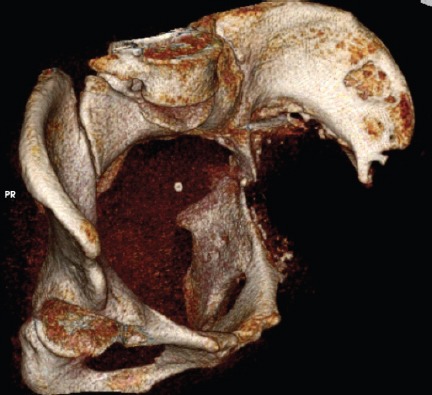
40 years female presented with inadequately managed transverse fracture of left acetabulum done by anterior extended ilio-inguinal approach. The fixation failed. She presented 6 months later with painful hip. Cemented total hip replacement was performed with reconstruction of acetabulum by posterior column plating. Six months postoperatively patient presented with dislodgement of cup, pelvic discontinuity and sinus in the thigh. Two stage revision surgery was planned. First implant, removal; debridement and antibiotic spacer surgery was performed. At second stage of revision total hip replacement, patient had Paprosky grade IIIb defect in acetabulum. Spacer was removed through the posterior approach. Anterior approach was taken for anterior plating. Intra-operatively external iliac pulsations were found to be absent so procedure was abandoned after expert opinion. Postoperatively digital subtraction angiography demonstrated a chronic block in the external iliac artery and corona mortis was the only patent vascular channel providing vascular to the left lower limb. Thus, peripheral limb was stealing blood supply from the acetabulum to maintain perfusion. Patient was ultimately left with pelvic discontinuity, excision arthroplasty and pseudoarthrosis of the left hip.
Avascular necrosis of acetabulum is a rare entity & often not recognized. One should be suspicious about diagnosis of avascular necrosis of acetabulum in select cases of failed acetabular fixation, previously operated via extensile anterior ilio - inguinal approach. Angiographic evaluation is essential in revision cases of failed acetabular fixation. Corona mortis (crown or circle of death) can sometimes act as a savior of limb.
髋臼的血供丰富,发生缺血性坏死的几率很低。但髋臼后柱骨折后创伤性髋臼缺血性坏死的病例已有充分记载。在髋臼骨折内固定失败的病例中,对于曾采用扩大入路(如扩大的髂股前入路或三放射状入路)进行手术的患者,识别和怀疑髋臼缺血性坏死至关重要。这类患者通常表现为反复的深部骨感染,或内固定早期失败伴假体无菌性松动及移位。我们报告一例类似病例。
一名40岁女性,因左侧髋臼横行骨折采用扩大的髂腹股沟前入路治疗,治疗效果不佳。内固定失败。6个月后她因髋关节疼痛前来就诊。行骨水泥型全髋关节置换术,同时采用后柱钢板重建髋臼。术后6个月,患者出现髋臼杯脱位、骨盆连续性中断及大腿窦道。计划进行两期翻修手术。第一期进行取出植入物、清创及抗生素间隔物手术。在翻修全髋关节置换术的第二期,患者髋臼出现Paprosky IIIb级缺损。通过后入路取出间隔物。采用前入路进行前路钢板固定。术中发现髂外动脉搏动消失,经专家会诊后放弃手术。术后数字减影血管造影显示髂外动脉慢性阻塞,死亡冠是唯一为左下肢供血的通畅血管通道。因此,外周肢体从髋臼窃取血液供应以维持灌注。患者最终遗留骨盆连续性中断、左髋关节切除成形术及假关节形成。
髋臼缺血性坏死是一种罕见疾病,常未被认识。在某些髋臼固定失败且此前采用扩大的髂腹股沟前入路手术的病例中,应怀疑髋臼缺血性坏死的诊断。血管造影评估在髋臼固定失败的翻修病例中至关重要。死亡冠有时可成为肢体的救星。