de Siqueira Maria Eduarda Menezes, Pozo Eduardo, Fernandes Veronica R, Sengupta Partho P, Modesto Karen, Gupta Sushilkumar Satish, Barbeito-Caamaño Cayetana, Narula Jagat, Fuster Valentin, Caixeta Adriano, Sanz Javier
The Zena and Michael A. Wiener Cardiovascular Institute/Marie-Josée and Henry R. Kravis Center for Cardiovascular Health, Icahn School of Medicine at Mount Sinai, New York, NY, USA.
Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, Brazil.
J Cardiovasc Magn Reson. 2016 Jun 16;18(1):39. doi: 10.1186/s12968-016-0258-x.
Prognosis in pulmonary hypertension (PH) is related to right ventricular (RV) function. Quantification of RV mechanics may offer additive value. The objective of our study is to determine the feasibility and clinical and prognostic value of RV strain analysis by cardiovascular magnetic resonance (CMR) based feature tracking (FT) in PH.
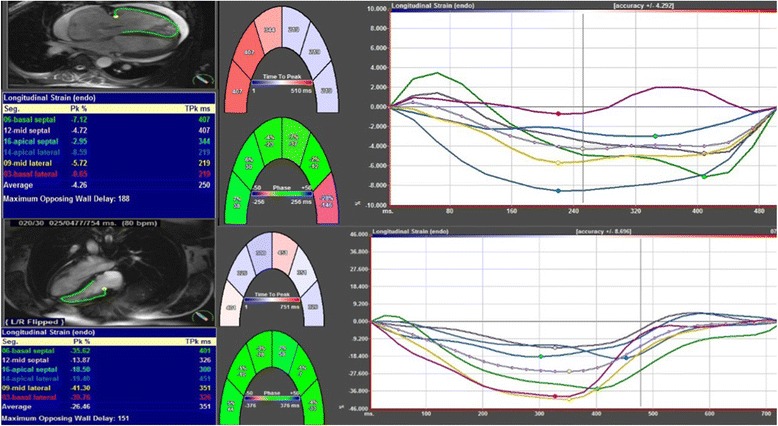
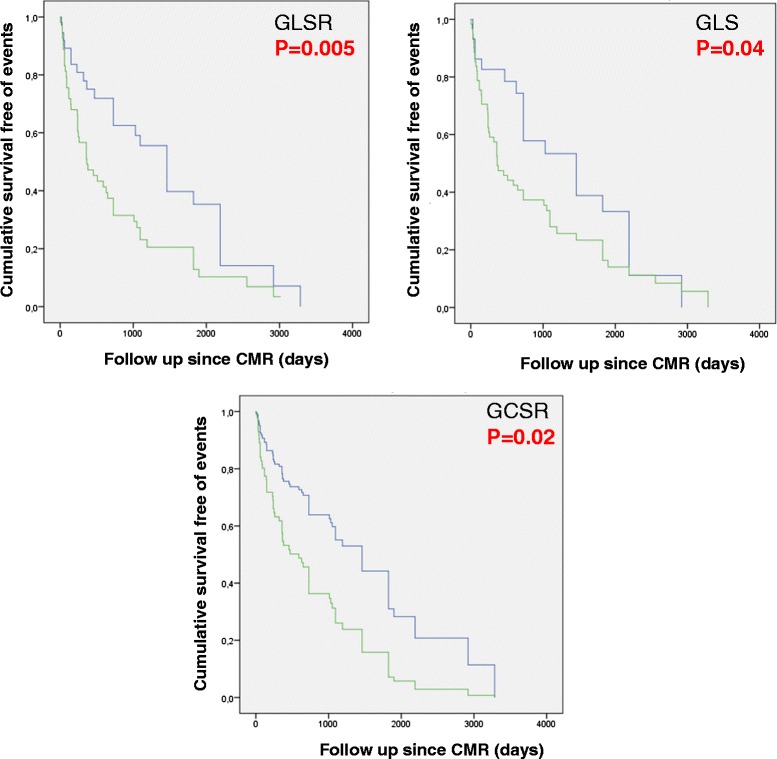
We retrospectively enrolled 116 patients (age 52.2 ± 12 years, 73.6 % women) referred to CMR for PH evaluation who underwent right heart catheterization within 1 month. Using dedicated FT software, peak global longitudinal and circumferential RV strain and strain rates (GLS, GCS, GLSR, and GCSR, respectively) were quantified from standard cine images. Using multivariate regression analysis, we evaluated the associations of strain with a composite endpoint of death, lung transplantation, or functional class deterioration.
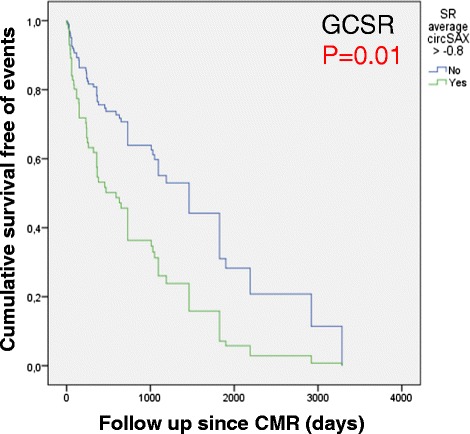
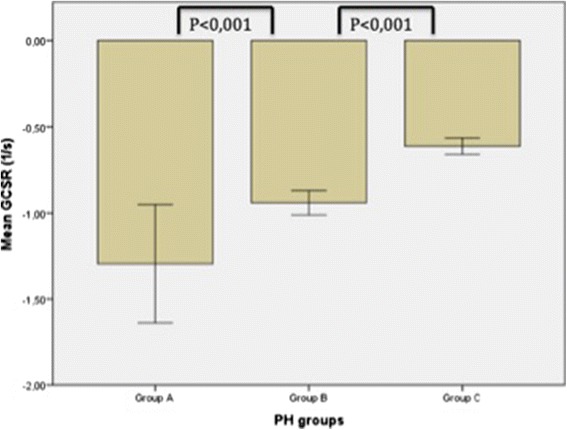
RV strain analysis was feasible in 110 (95 %) patients. Patients were classified into: Group A (no PH, normal right ventricular ejection fraction [RVEF]; n = 17), Group B (PH, normal RVEF; n = 26), or Group C (PH, abnormal RVEF; n = 67). All strain and strain rate values were reduced in Group C. Furthermore, GCSR was significantly reduced in Group B (-0.92 [-1.0/-0.7]; p < 0.001) compared to Group A (-1.12 [-1.3/-0.9]; p < 0.001). After adjustment for six clinically meaningful covariates, GLS (hazard ratio 1.06; p = 0.026), GLSR (hazard ratio 2.52; p = 0.04), and GCSR (hazard ratio 4.5; p = 0.01) were independently associated with the composite endpoint. GCSR successfully discriminated patients with and without events (p = 0.01).
Quantification of RV strain with CMR-FT is feasible in the majority of patients, correlates with disease severity, and is independently associated with poor outcomes in PH.
肺动脉高压(PH)的预后与右心室(RV)功能有关。右心室力学的量化可能具有附加价值。我们研究的目的是确定基于心血管磁共振(CMR)特征追踪(FT)的右心室应变分析在PH中的可行性、临床及预后价值。
我们回顾性纳入了116例因PH评估而接受CMR检查且在1个月内进行了右心导管检查的患者(年龄52.2±12岁,73.6%为女性)。使用专用的FT软件,从标准电影图像中量化右心室整体纵向和圆周应变及应变率(分别为GLS、GCS、GLSR和GCSR)。使用多变量回归分析,我们评估了应变与死亡、肺移植或功能分级恶化的复合终点之间的关联。
110例(95%)患者可行右心室应变分析。患者被分为:A组(无PH,右心室射血分数[RVEF]正常;n = 17)、B组(PH,RVEF正常;n = 26)或C组(PH,RVEF异常;n = 67)。C组所有应变和应变率值均降低。此外,与A组(-1.12[-1.3/-0.9];p < 0.001)相比,B组的GCSR显著降低(-0.92[-1.0/-0.7];p < 0.001)。在对六个具有临床意义的协变量进行调整后,GLS(风险比1.06;p = 0.026)、GLSR(风险比2.52;p = 0.04)和GCSR(风险比4.5;p = 0.01)与复合终点独立相关。GCSR成功区分了有事件和无事件的患者(p = 0.01)。
在大多数患者中,使用CMR-FT量化右心室应变是可行的,与疾病严重程度相关,并且在PH中与不良预后独立相关。