Johnson Peter, Federico Massimo, Kirkwood Amy, Fosså Alexander, Berkahn Leanne, Carella Angelo, d'Amore Francesco, Enblad Gunilla, Franceschetto Antonella, Fulham Michael, Luminari Stefano, O'Doherty Michael, Patrick Pip, Roberts Thomas, Sidra Gamal, Stevens Lindsey, Smith Paul, Trotman Judith, Viney Zaid, Radford John, Barrington Sally
From the Cancer Research UK Centre, University of Southampton, Southampton (P.J.), Cancer Research UK and University College London Cancer Trials Centre (A.K., P.P., T.R., L.S., P.S.) and the PET Imaging Centre, King's College London, King's Health Partners, St. Thomas' Hospital (M.O., Z.V., S.B.), London, the Department of Haematology, Lincoln County Hospital, Lincoln (G.S.), and the Department of Medical Oncology, Christie Hospital, Manchester (J.R.) - all in the United Kingdom; the Department of Diagnostic, Clinical, and Public Health Medicine, University of Modena and Reggio Emilia, Modena (M. Federico, A. Franceschetto, S.L.), the Department of Hematology, San Martino University Hospital, Genoa (A.C.), and Arcispedale Santa Maria Nuova-Istituti di Ricovero e Cura a Carattere Scientifico, Reggio Emilia (S.L.) - all in Italy; the Department of Medical Oncology, Oslo University Hospital, Oslo (A. Fosså); the Department of Haematology, Auckland City Hospital, Auckland, New Zealand (L.B.); the Department of Hematology, Aarhus University Hospital, Aarhus, Denmark (F.A.); the Department of Immunology, Genetics, and Pathology, Uppsala University, Uppsala, Sweden (G.E.); and the Department of Molecular Imaging, Royal Prince Alfred Hospital (M. Fulham), and Concord Repatriation General Hospital, University of Sydney (J.T.), Sydney.
N Engl J Med. 2016 Jun 23;374(25):2419-29. doi: 10.1056/NEJMoa1510093.
We tested interim positron-emission tomography-computed tomography (PET-CT) as a measure of early response to chemotherapy in order to guide treatment for patients with advanced Hodgkin's lymphoma.
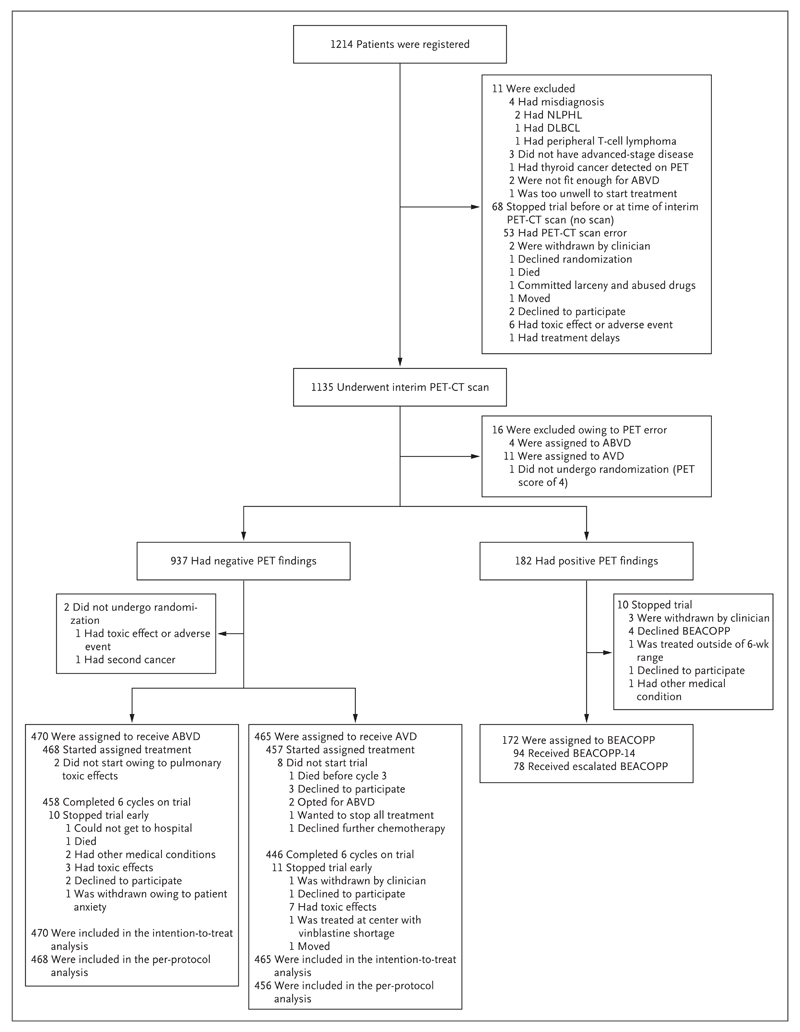
Patients with newly diagnosed advanced classic Hodgkin's lymphoma underwent a baseline PET-CT scan, received two cycles of ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) chemotherapy, and then underwent an interim PET-CT scan. Images were centrally reviewed with the use of a 5-point scale for PET findings. Patients with negative PET findings after two cycles were randomly assigned to continue ABVD (ABVD group) or omit bleomycin (AVD group) in cycles 3 through 6. Those with positive PET findings after two cycles received BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone). Radiotherapy was not recommended for patients with negative findings on interim scans. The primary outcome was the difference in the 3-year progression-free survival rate between randomized groups, a noninferiority comparison to exclude a difference of 5 or more percentage points.
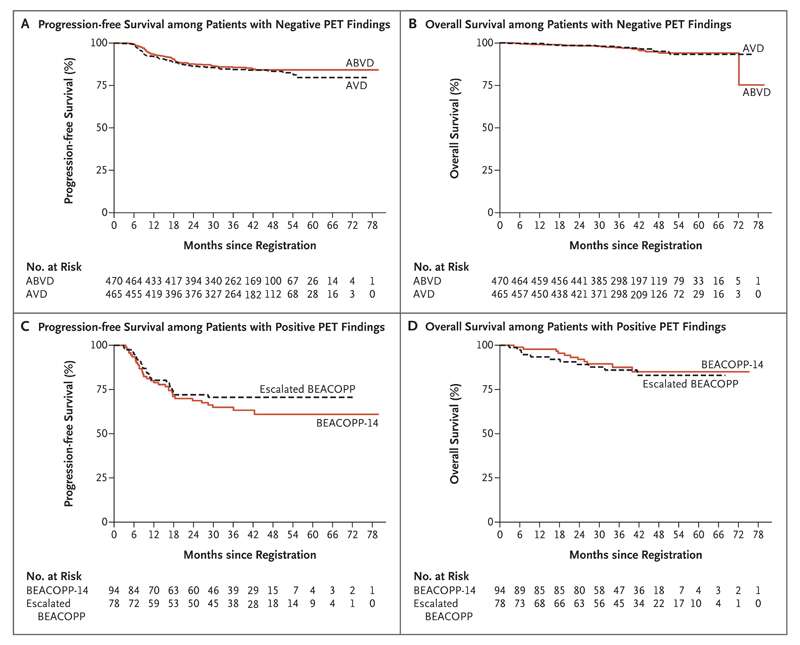
A total of 1214 patients were registered; 937 of the 1119 patients (83.7%) who underwent an interim PET-CT scan according to protocol had negative findings. With a median follow-up of 41 months, the 3-year progression-free survival rate and overall survival rate in the ABVD group were 85.7% (95% confidence interval [CI], 82.1 to 88.6) and 97.2% (95% CI, 95.1 to 98.4), respectively; the corresponding rates in the AVD group were 84.4% (95% CI, 80.7 to 87.5) and 97.6% (95% CI, 95.6 to 98.7). The absolute difference in the 3-year progression-free survival rate (ABVD minus AVD) was 1.6 percentage points (95% CI, -3.2 to 5.3). Respiratory adverse events were more severe in the ABVD group than in the AVD group. BEACOPP was given to the 172 patients with positive findings on the interim scan, and 74.4% had negative findings on a third PET-CT scan; the 3-year progression-free survival rate was 67.5% and the overall survival rate 87.8%. A total of 62 patients died during the trial (24 from Hodgkin's lymphoma), for a 3-year progression-free survival rate of 82.6% and an overall survival rate of 95.8%.
Although the results fall just short of the specified noninferiority margin, the omission of bleomycin from the ABVD regimen after negative findings on interim PET resulted in a lower incidence of pulmonary toxic effects than with continued ABVD but not significantly lower efficacy. (Funded by Cancer Research UK and Others; ClinicalTrials.gov number, NCT00678327.).
我们对中期正电子发射断层扫描-计算机断层扫描(PET-CT)作为晚期霍奇金淋巴瘤患者化疗早期反应的一种测量方法进行了测试,以指导治疗。
新诊断的晚期经典霍奇金淋巴瘤患者接受基线PET-CT扫描,接受两个周期的ABVD(多柔比星、博来霉素、长春花碱和达卡巴嗪)化疗,然后进行中期PET-CT扫描。使用5分制对PET结果进行集中审查。两个周期后PET结果为阴性的患者被随机分配在第3至6周期继续使用ABVD(ABVD组)或省略博来霉素(AVD组)。两个周期后PET结果为阳性的患者接受BEACOPP(博来霉素、依托泊苷、多柔比星、环磷酰胺、长春新碱、丙卡巴肼和泼尼松)。中期扫描结果为阴性的患者不建议进行放疗。主要结局是随机分组组之间3年无进展生存率的差异,这是一项非劣效性比较,以排除差异达5个或更多百分点的情况。
共登记了1214例患者;按照方案进行中期PET-CT扫描的1119例患者中有937例(83.7%)结果为阴性。中位随访41个月时,ABVD组的3年无进展生存率和总生存率分别为85.7%(95%置信区间[CI],82.1至88.6)和97.2%(95%CI,95.1至98.4);AVD组的相应比率分别为84.4%(95%CI,80.7至87.5)和97.6%(95%CI,95.6至98.)。3年无进展生存率的绝对差异(ABVD减去AVD)为1.6个百分点(95%CI,-3.2至5.3)。ABVD组的呼吸不良事件比AVD组更严重。中期扫描结果为阳性的172例患者接受了BEACOPP治疗,74.4%的患者在第三次PET-CT扫描时结果为阴性;3年无进展生存率为67.5%,总生存率为87.8%。共有62例患者在试验期间死亡(24例死于霍奇金淋巴瘤),3年无进展生存率为82.6%,总生存率为95.8%。
尽管结果略未达到规定的非劣效性界限,但中期PET结果为阴性后ABVD方案中省略博来霉素导致肺部毒性发生率低于继续使用ABVD,但疗效降低不显著。(由英国癌症研究基金会及其他机构资助;ClinicalTrials.gov编号,NCT00678327。)