Storm Ilse, den Hertog Frank, van Oers Hans, Schuit Albertine J
National Institute for Public Health and the Environment, Centre for Health and Society, PO Box 1, 3720 BA, Bilthoven, The Netherlands.
Tilburg University, Tranzo Scientific Center for Care and Welfare, PO 90153, 5000 LE, Tilburg, The Netherlands.
Int J Equity Health. 2016 Jun 22;15:97. doi: 10.1186/s12939-016-0384-y.
The causes of health inequalities are complex. For the reduction of health inequalities, intersectoral collaboration between the public health sector and both social policy sectors (e.g. youth affairs, education) and physical policy sectors (e.g. housing, spatial planning) is essential, but in local practice difficult to realize. The aim of this study was to examine the collaboration between the sectors in question more closely and to identify opportunities for improvement.
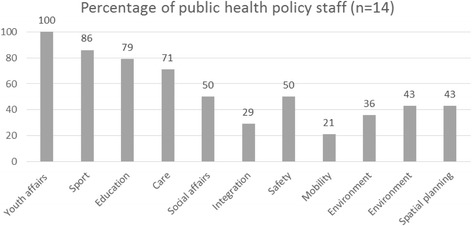
A qualitative descriptive analysis of five aspects of collaboration within sixteen Dutch municipalities was performed to examine the collaboration between the public health sector and other policy sectors: 1) involvement of the sectors in the public health policy network, 2) harmonisation of objectives, 3) use of policies by the relevant sectors, 4) formalised collaboration, and 5) previous experience. Empirical data on these collaboration aspects were collected based on document analysis, questionnaires and interviews.
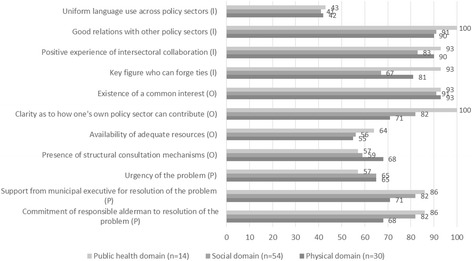
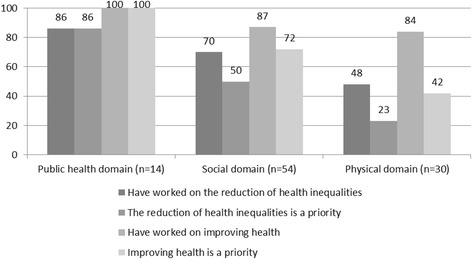
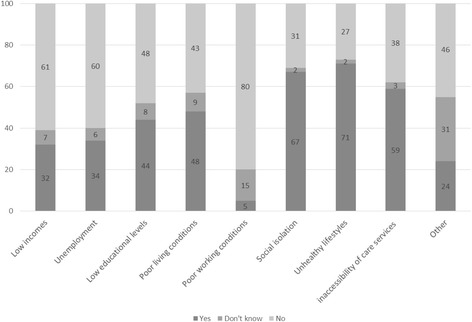
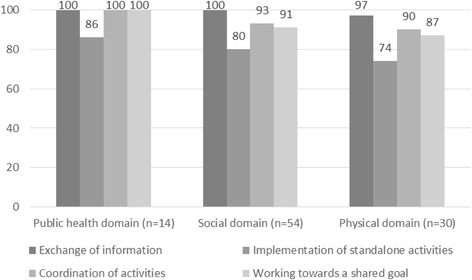
The study found that the policy workers of social sectors were more involved in the public health network and more frequently supported the objectives in the field of health inequality reduction. Both social policy sectors and physical policy sectors used policies and activities to reduce health inequalities. More is done to influence the determinants of health inequality through policies aimed at lifestyle and social setting than through policies aimed at socioeconomic factors and the physical environment. Where the physical policy sectors are involved in the public health network, the collaboration follows a very similar pattern as with the social policy sectors. All sectors recognise the importance of good relationships, positive experiences, a common interest in working together and coordinated mechanisms.
This study shows that there is scope for improving collaboration in the field of health inequality reduction between the public health sector and both social policy sectors and physical policy sectors. Ways in which improvement could be realised include involving physical policy sectors in the network, pursuing widely supported policy goals, making balanced efforts to influence determinants of health inequalities, and increasing the emphasis on a programmatic approach.
健康不平等的成因复杂。为减少健康不平等,公共卫生部门与社会政策部门(如青年事务、教育)和物质环境政策部门(如住房、空间规划)之间的跨部门合作至关重要,但在地方实践中难以实现。本研究旨在更深入地考察相关部门之间的合作,并找出改进的机会。
对荷兰16个城市合作的五个方面进行定性描述分析,以考察公共卫生部门与其他政策部门之间的合作:1)各部门在公共卫生政策网络中的参与情况;2)目标的协调一致;3)相关部门对政策的运用;4)正式合作;5)以往经验。基于文献分析、问卷调查和访谈收集了关于这些合作方面的实证数据。
研究发现,社会部门的政策工作者更多地参与公共卫生网络,且更频繁地支持减少健康不平等领域的目标。社会政策部门和物质环境政策部门都运用政策和活动来减少健康不平等。通过针对生活方式和社会环境的政策来影响健康不平等的决定因素,比通过针对社会经济因素和物质环境的政策做得更多。在物质环境政策部门参与公共卫生网络的地方,合作模式与社会政策部门非常相似。所有部门都认识到良好关系、积极经验、合作的共同利益以及协调机制的重要性。
本研究表明,在减少健康不平等领域,公共卫生部门与社会政策部门和物质环境政策部门之间的合作仍有改进空间。实现改进的方式包括让物质环境政策部门参与网络、追求得到广泛支持的政策目标、平衡努力以影响健康不平等的决定因素,以及更加注重采用规划性方法。