Uwingabiye Jean, Frikh Mohammed, Lemnouer Abdelhay, Bssaibis Fatna, Belefquih Bouchra, Maleb Adil, Dahraoui Souhail, Belyamani Lahcen, Bait Abdelouahed, Haimeur Charki, Louzi Lhoussain, Ibrahimi Azeddine, Elouennass Mostafa
Service de Bactériologie, Hôpital Militaire d'Instruction Mohammed V, Rabat, Maroc; Equipe de recherche: Épidémiologie et Résistance Bactérienne (ERB), Université Mohammed V, Faculté de Médecine et de Pharmacie, Rabat, Maroc.
Service de Bactériologie, Hôpital Militaire d'Instruction Mohammed V, Rabat, Maroc.
Pan Afr Med J. 2016 Apr 15;23:191. doi: 10.11604/pamj.2016.23.191.7915. eCollection 2016.
This study aims to determine the Acinetobacter sp clinical isolates frequency and its antibiotic susceptibility pattern by comparing results obtained from the Intensive Care Units (ICUs) to that of other units at the Mohammed V Military Teaching Hospital in Rabat.
This is a retrospective study over a 2-years period where we collected all clinical isolates of Acinetobacter sp obtained from samples for infection diagnosis performed on hospitalized patients between 2012 to 2014.
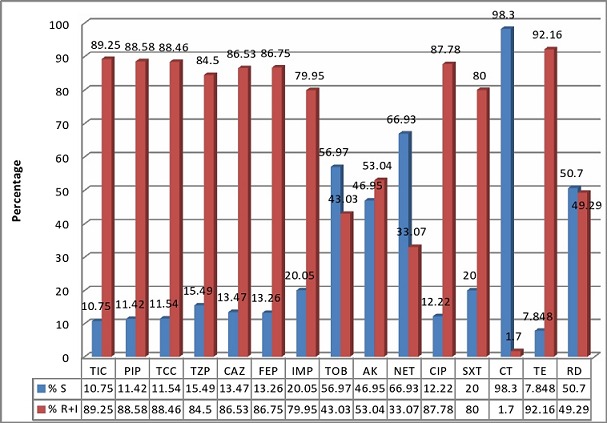
During the study period, 441 clinical and non-repetitive isolates of Acinetobacter sp were collected representing 6.94% of all bacterial clinical isolates (n = 6352) and 9.6% of Gram negative rods (n = 4569). More than a half of the isolates were from the ICUs and were obtained from 293 infected patients of which 65, 2% (191 cases) were males (sex ratio = 1.9) and the median age was 56 years (interquartile range: 42-68 years). Acinetobacter clinical isolates were obtained from respiratory samples (44.67%) followed by blood cultures (14.51%). The resistance to ciprofloxacin, ceftazidime, piperacillin / tazobactam, imipenem, amikacin, tobramycin, netilmicin, rifampicin and colistin was respectively 87%, 86%, 79%, 76%; 52%, 43%, 33% 32% and 1.7%. The difference in resistance between the ICUs and the other units was statistically significant (p <0.05) except for colistin, tetracycline and rifampicin.
This paper shows that solving the problem of prevalence and high rate of multidrug resistant Acinetobacter infection which represents a therapeutic impasse, requires the control of the hospital environment and optimizing hands hygiene and antibiotics use in the hospital.
本研究旨在通过比较拉巴特穆罕默德五世军事教学医院重症监护病房(ICU)与其他科室的结果,确定不动杆菌属临床分离株的频率及其抗生素敏感性模式。
这是一项为期2年的回顾性研究,我们收集了2012年至2014年期间从住院患者感染诊断样本中获得的所有不动杆菌属临床分离株。
在研究期间,共收集到441株临床非重复性不动杆菌属分离株,占所有细菌临床分离株(n = 6352)的6.94%,占革兰氏阴性杆菌(n = 4569)的9.6%。超过一半的分离株来自ICU,来自293例感染患者,其中65.2%(191例)为男性(性别比 = 1.9),中位年龄为56岁(四分位间距:42 - 68岁)。不动杆菌临床分离株来自呼吸道样本(44.67%),其次是血培养(14.51%)。对环丙沙星、头孢他啶、哌拉西林/他唑巴坦、亚胺培南、阿米卡星、妥布霉素、奈替米星、利福平和黏菌素的耐药率分别为87%、86%、79%、76%、52%、43%、33%、32%和1.7%。除黏菌素、四环素和利福平外,ICU与其他科室之间的耐药差异具有统计学意义(p <0.05)。
本文表明,解决多重耐药不动杆菌感染的流行问题及其高发生率这一治疗难题,需要控制医院环境并优化医院的手卫生和抗生素使用。