Safdar Basmah, D'Onofrio Gail
Department of Emergency Medicine Yale University School of Medicine, New Haven CT.
Yale J Biol Med. 2016 Jun 27;89(2):227-38. eCollection 2016 Jun.
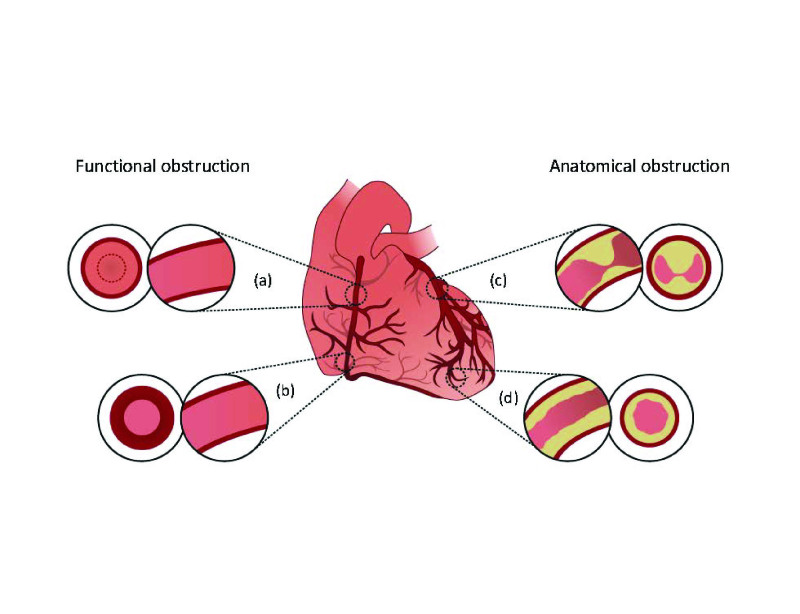
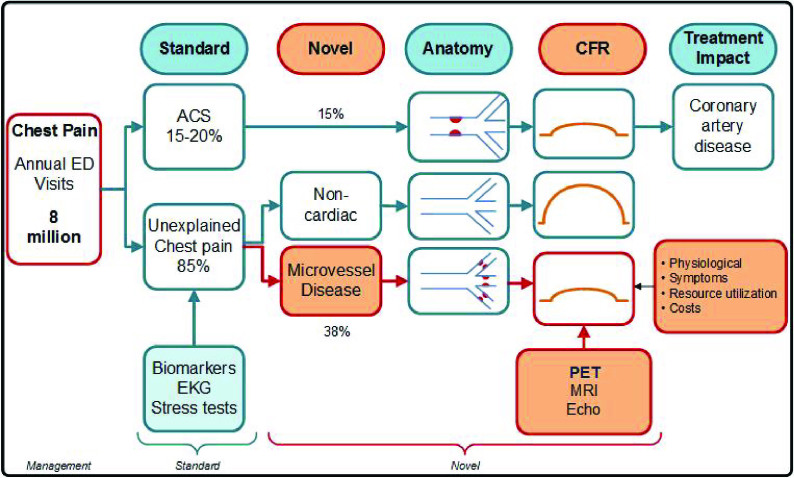
Emergency departments (ED) in the United States see over eight million cases of chest pain annually. While a cardinal symptom of acute coronary syndrome (ACS), multiple emergent and non-emergent causes can attribute to chest pain. This case-based perspective describes the different sex-specific causes of angina seen in ED patients. Once coronary artery disease (CAD) is ruled out with standard protocols, microvascular dysfunction is perhaps the most prevalent but under-diagnosed cause of non-CAD related angina in ED patients. Additional causes include coronary artery spasm, coronary artery dissection, coronary artery endothelial dysfunction and myocardial bridging. Non-CAD related angina is associated with persistent chest pain causing poor function, quality of life, and recidivism. Clinicians should consider additional diagnostics to routinely screen for non-CAD related causes of angina in patients with recurrent chest pain. Future work is needed to better define the epidemiological, clinical, biological, and genetic correlates of microvascular dysfunction in these patients.
美国急诊科每年接诊超过800万例胸痛病例。虽然胸痛是急性冠状动脉综合征(ACS)的主要症状,但多种紧急和非紧急病因都可能导致胸痛。本文基于病例探讨了急诊科患者中不同性别特异性的心绞痛病因。一旦通过标准方案排除冠状动脉疾病(CAD),微血管功能障碍可能是急诊科患者中非CAD相关心绞痛最常见但诊断不足的病因。其他病因包括冠状动脉痉挛、冠状动脉夹层、冠状动脉内皮功能障碍和心肌桥。非CAD相关心绞痛与持续性胸痛相关,可导致功能不佳、生活质量下降和复发。临床医生应考虑采用其他诊断方法,对复发性胸痛患者常规筛查非CAD相关的心绞痛病因。未来需要开展更多工作,以更好地明确这些患者微血管功能障碍的流行病学、临床、生物学和遗传学关联。