Vidler Marianne, Ramadurg Umesh, Charantimath Umesh, Katageri Geetanjali, Karadiguddi Chandrashekhar, Sawchuck Diane, Qureshi Rahat, Dharamsi Shafik, Joshi Anjali, von Dadelszen Peter, Derman Richard, Bellad Mrutyunjaya, Goudar Shivaprasad, Mallapur Ashalata
Department of Obstetrics and Gynaecology, and the Child and Family Research Unit, University of British Columbia, Vancouver, BC, Canada.
Department of Community Medicine, S Nijalingappa Medical College, Bagalkot, Karnataka, India.
Reprod Health. 2016 Jun 8;13 Suppl 1(Suppl 1):37. doi: 10.1186/s12978-016-0138-8.
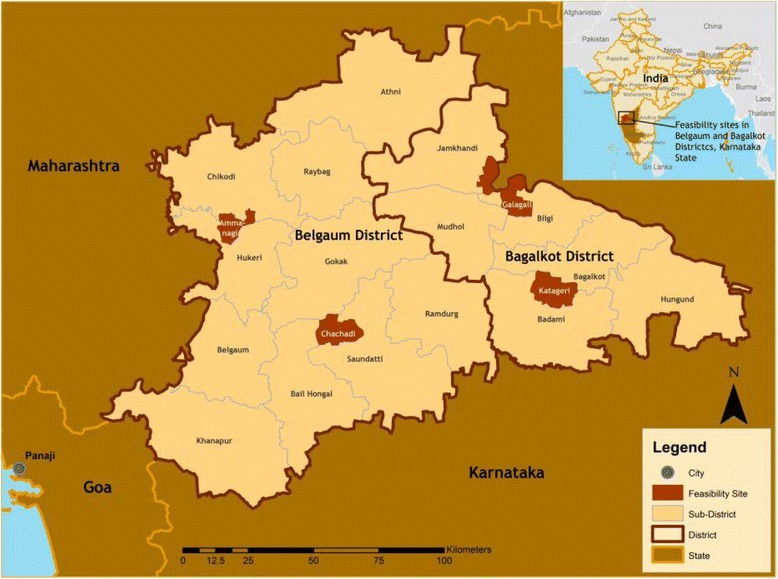
Karnataka State continues to have the highest rates of maternal mortality in south India at 144/100,000 live births, but lower than the national estimates of 190-220/100,000 live births. Various barriers exist to timely and appropriate utilization of services during pregnancy, childbirth and postpartum. This study aimed to describe the patterns and determinants of routine and emergency maternal health care utilization in rural Karnataka State, India.
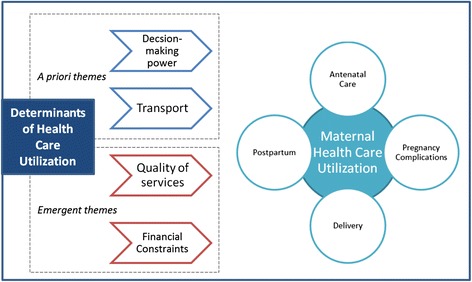
This study was conducted in Karnataka in 2012-2013. Purposive sampling was used to convene twenty three focus groups and twelve individual interviews with community and health system representatives: Auxiliary Nurse Midwives and Staff Nurses, Accredited Social Health Activists, community leaders, male decision-makers, female decision-makers, women of reproductive age, medical officers, private health care providers, senior health administrators, District health officers, and obstetricians. Local researchers familiar with the setting and language conducted all focus groups and interviews, these researchers were not known to community participants. All discussions were audio recorded, transcribed, and translated to English for analysis. A thematic analysis approach was taken utilizing an a priori thematic framework as well as inductive identification of themes.
Most women in the focus groups reported regular antenatal care attendance, for an average of four visits, and more often for high-risk pregnancies. Antenatal care was typically delivered at the periphery by non-specialised providers. Participants reported that sought was care women experienced danger signs of complications. Postpartum care was reportedly rare, and mainly sought for the purpose of neonatal care. Factors that influenced women's care-seeking included their limited autonomy, poor access to and funding for transport for non-emergent conditions, perceived poor quality of health care facilities, and the costs of care.
Rural south Indian communities reported regular use of health care services during pregnancy and for delivery. Uptake of maternity care services was attributed to new government programmes and increased availability of maternity services; nevertheless, some women delayed disclosure of pregnancy and first antenatal visit. Community-based initiatives should be enhanced to encourage early disclosure of pregnancies and to provide the community information regarding the importance of facility-based care. Health facility infrastructure in rural Karnataka should also be enhanced to ensure a consistent power supply and improved cleanliness on the wards.
NCT01911494.
卡纳塔克邦仍是印度南部孕产妇死亡率最高的地区,为每10万例活产中有144例死亡,但低于全国估计的每10万例活产190 - 220例的死亡率。在孕期、分娩期和产后及时且恰当地利用医疗服务存在各种障碍。本研究旨在描述印度卡纳塔克邦农村地区常规和紧急孕产妇保健服务利用的模式及决定因素。
本研究于2012 - 2013年在卡纳塔克邦开展。采用目的抽样法召集了23个焦点小组,并对社区和卫生系统代表进行了12次个人访谈,这些代表包括辅助护士助产士和注册护士、经认可的社会健康活动家、社区领袖、男性决策者、女性决策者、育龄妇女、医务人员、私人医疗服务提供者、高级卫生管理人员、地区卫生官员和产科医生。熟悉当地情况和语言的当地研究人员进行了所有焦点小组讨论和访谈,社区参与者不认识这些研究人员。所有讨论均进行了录音、转录,并翻译成英文进行分析。采用主题分析方法,利用先验主题框架以及归纳主题识别。
焦点小组中的大多数女性报告称定期进行产前检查,平均就诊4次,高危妊娠的就诊频率更高。产前检查通常由非专业人员在基层提供。参与者报告称,女性寻求护理是因为她们出现了并发症的危险信号。据报道,产后护理很少见,主要是为了新生儿护理而寻求。影响女性寻求护理的因素包括她们自主权有限、非紧急情况下交通不便且缺乏交通费用、认为医疗设施质量差以及护理费用。
印度南部农村社区报告称在孕期和分娩时经常使用医疗服务。孕产妇保健服务的利用归因于新的政府项目和孕产妇服务可及性的提高;然而,一些女性推迟透露怀孕情况和首次产前检查。应加强基于社区的举措,以鼓励尽早透露怀孕情况,并向社区提供有关设施分娩护理重要性的信息。卡纳塔克邦农村地区的医疗机构基础设施也应得到加强,以确保持续供电并改善病房清洁状况。
NCT01911494。