Bourcier Simon, Pichereau Claire, Boelle Pierre-Yves, Nemlaghi Safaa, Dubée Vincent, Lejour Gabriel, Baudel Jean-Luc, Galbois Arnaud, Lavillegrand Jean-Rémi, Bigé Naïke, Tahiri Jalel, Leblanc Guillaume, Maury Eric, Guidet Bertrand, Ait-Oufella Hafid
Service de réanimation médicale, Hôpital Saint-Antoine, Assistance Publique-Hôpitaux de Paris (AP-HP), 184 rue du Faubourg Saint-Antoine, 75571, Paris Cedex 12, France.
Université Pierre et Marie Curie-Paris 6, Paris, France.
Ann Intensive Care. 2016 Dec;6(1):63. doi: 10.1186/s13613-016-0164-2. Epub 2016 Jul 11.
Microcirculatory disorders leading to tissue hypoperfusion play a central role in the pathophysiology of organ failure in severe sepsis and septic shock. As microcirculatory disorders have been identified as strong predictive factors of unfavourable outcome, there is a need to develop accurate parameters at the bedside to evaluate tissue perfusion. We evaluated whether different body temperature gradients could relate to sepsis severity and could predict outcome in critically ill patients with severe sepsis and septic shock.
We conducted a prospective observational study in a tertiary teaching hospital in France. During a 10-month period, all consecutive adult patients with severe sepsis or septic shock who required ICU admission were included. Six hours after initial resuscitation (H6), we recorded the hemodynamic parameters and four temperature gradients: central-to-toe, central-to-knee, toe-to-room and knee-to-room.
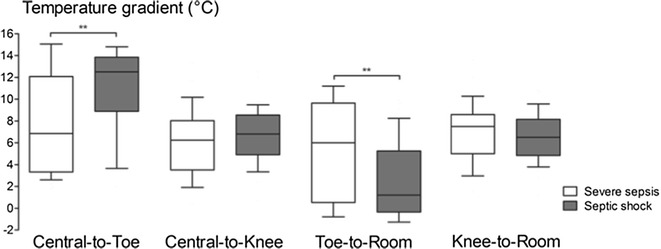
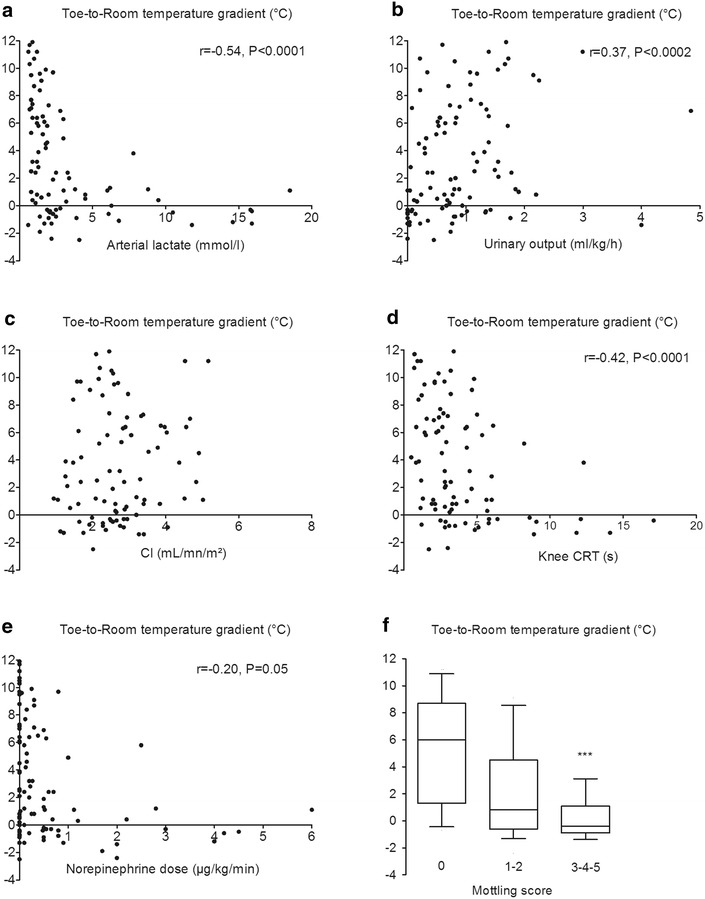
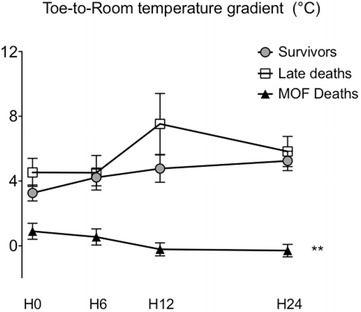
We evaluated 40 patients with severe sepsis (40/103, 39 %) and 63 patients with septic shock (63/103, 61 %). In patients with septic shock, central-to-toe temperature gradient was significantly higher (12.5 [9.2; 13.8] vs 6.9 [3.4; 12.0] °C, P < 0.001) and toe-to-room temperature gradient significantly lower (1.2 [-0.3; 5.2] vs 6.0 [0.6; 9.5] °C, P < 0.001) than in patients with severe sepsis. Overall ICU mortality rate due to multiple organ failure (MOF) was 21 %. After initial resuscitation, toe-to-room temperature gradient was significantly lower in patients dead from MOF than in the survivors (-0.2 [-1.1; +1.3] °C vs +3.9 [+0.5; +7.2] °C, P < 0.001) and the difference in gradients increased during the first 24 h. Furthermore, toe-to-room temperature gradient was related to tissue perfusion parameters such as arterial lactate level (r = -0.54, P < 0.0001), urine output (r = 0.37, P = 0.0002), knee capillary refill time (r = -0.42, P < 0.0001) and mottling score (P = 0.001).
Toe-to-room temperature gradient reflects tissue perfusion at the bedside and is a strong prognosis factor in critically ill patients with severe infections.
导致组织灌注不足的微循环障碍在严重脓毒症和脓毒性休克所致器官功能衰竭的病理生理过程中起核心作用。由于微循环障碍已被确定为不良预后的强预测因素,因此需要开发床旁准确参数来评估组织灌注。我们评估了不同的体温梯度是否与脓毒症严重程度相关,以及能否预测严重脓毒症和脓毒性休克重症患者的预后。
我们在法国一家三级教学医院进行了一项前瞻性观察研究。在10个月期间,纳入了所有连续入住重症监护病房(ICU)的严重脓毒症或脓毒性休克成年患者。初始复苏6小时后(H6),我们记录了血流动力学参数和四个体温梯度:中心至趾端、中心至膝部、趾端至病房和膝部至病房。
我们评估了40例严重脓毒症患者(40/103,39%)和63例脓毒性休克患者(63/103,61%)。在脓毒性休克患者中,中心至趾端体温梯度显著更高(12.5 [9.2;13.8]℃ 对 6.9 [3.4;12.0]℃,P < 0.001),趾端至病房体温梯度显著更低(1.2 [-0.3;5.2]℃ 对 6.0 [0.6;9.5]℃,P < 0.001),与严重脓毒症患者相比。因多器官功能衰竭(MOF)导致的总体ICU死亡率为21%。初始复苏后,死于MOF的患者趾端至病房体温梯度显著低于幸存者(-0.2 [-1.1;+1.3]℃ 对 +3.9 [+0.5;+7.2]℃,P < 0.001),且梯度差异在最初24小时内增大。此外,趾端至病房体温梯度与组织灌注参数相关,如动脉血乳酸水平(r = -0.54,P < 0.0001)、尿量(r = 0.37,P = 0.0002)、膝部毛细血管再充盈时间(r = -0.42,P < 0.0001)和皮肤斑纹评分(P = 0.001)。
趾端至病房体温梯度反映了床旁组织灌注情况,是严重感染重症患者的一个强有力的预后因素。