Abe Ricardo Y, Diniz-Filho Alberto, Zangwill Linda M, Gracitelli Carolina P B, Marvasti Amir H, Weinreb Robert N, Baig Saif, Medeiros Felipe A
Invest Ophthalmol Vis Sci. 2016 Jul 1;57(9):OCT421-8. doi: 10.1167/iovs.15-18940.
The purpose of this study was to evaluate the effect of disease severity and number of tests acquired during follow-up on the relative odds of identifying progression by structural or functional tests in glaucoma.
This was an observational cohort study involving 462 eyes of 305 patients with glaucoma and 62 eyes of 49 healthy subjects. Glaucoma patients and healthy subjects were followed for an average of 3.6 ± 0.9 and 3.8 ± 0.9 years, with a median (interquantile range) of 8 (6-9) and 7 (6-8) visits, respectively. At each visit, subjects underwent visual field assessment with standard automated perimetry (SAP) and retinal nerve fiber layer (RNFL) evaluation by spectral-domain optical coherence tomography (SD-OCT). Slopes of change in SAP mean sensitivity and OCT RNFL thickness over time were estimated by linear regression using progressively cumulative visits over time. Cutoff values for age-related expected rates of change for each test were obtained from the healthy group. Progression by SD-OCT and/or SAP was determined if the slope of change was statistically significant and also lower (faster) than the fifth percentile cutoff calculated from the healthy group. A generalized estimating equation logistic regression model was used to evaluate the relative odds of progressing by OCT versus SAP in glaucoma eyes.
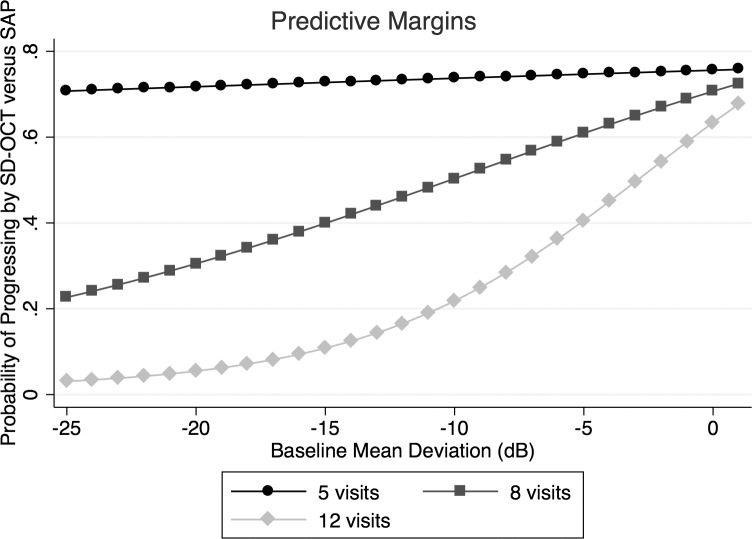
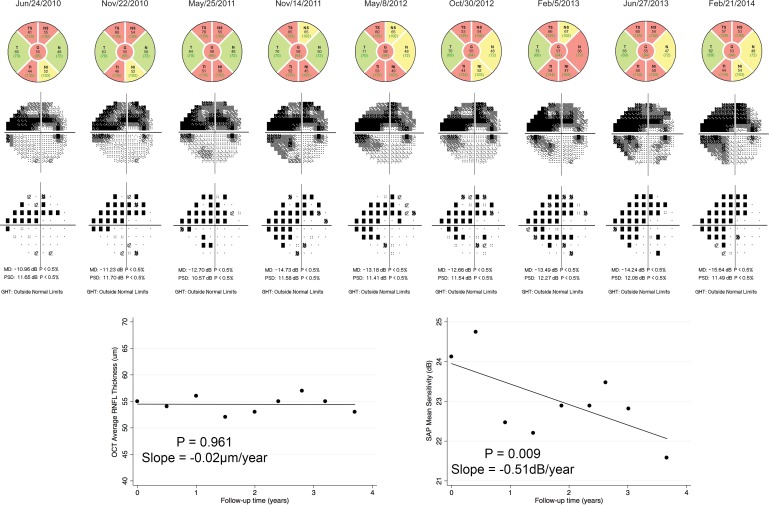
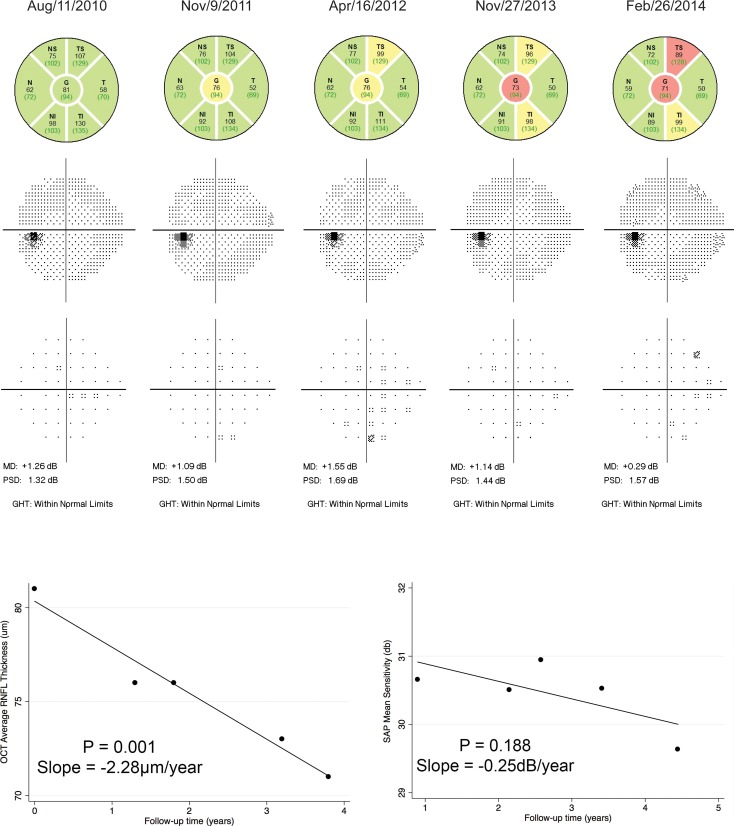
Eyes with less severe disease at baseline had a higher chance of being detected as progressing by SD-OCT but not by SAP, whereas an increase in disease severity at baseline increased the chance that the eye would be detected as progressing by SAP but not SD-OCT. Each 1 dB higher MD was associated with a 5% increase in the odds of detecting progression by SD-OCT versus SAP (odds ratio = 1.05 per 1 dB; 95% confidence interval: 1.01-1.09; P = 0.005).
The ability to detect glaucoma progression by SAP versus SD-OCT is significantly influenced by the stage of disease. Our results may provide useful information for guiding clinicians on the relative utility of these tests for detecting change throughout the disease continuum.
本研究旨在评估疾病严重程度以及随访期间所进行检查的数量对青光眼患者通过结构或功能检查识别病情进展的相对概率的影响。
这是一项观察性队列研究,纳入了305例青光眼患者的462只眼以及49名健康受试者的62只眼。青光眼患者和健康受试者的随访时间平均分别为3.6±0.9年和3.8±0.9年,中位数(四分位间距)分别为8(6 - 9)次和7(6 - 8)次就诊。每次就诊时,受试者均接受标准自动视野计(SAP)进行视野评估,并通过频域光学相干断层扫描(SD - OCT)评估视网膜神经纤维层(RNFL)。使用随时间逐步累积的就诊数据,通过线性回归估计SAP平均敏感度和OCT RNFL厚度随时间的变化斜率。从健康组获得每项检查与年龄相关的预期变化率的临界值。如果变化斜率具有统计学意义且低于从健康组计算出的第五百分位数临界值,则判定为通过SD - OCT和/或SAP出现病情进展。使用广义估计方程逻辑回归模型评估青光眼眼中通过OCT与SAP出现病情进展的相对概率。
基线时病情较轻的眼睛通过SD - OCT检测出病情进展的可能性较高,但通过SAP检测不出;而基线时病情严重程度增加,则眼睛通过SAP检测出病情进展的可能性增加,但通过SD - OCT检测不出。平均缺损(MD)每升高1 dB,通过SD - OCT检测出病情进展相对于SAP的概率增加5%(比值比 = 每1 dB为1.05;95%置信区间:1. .01 - 1.09;P = 0.005)。
通过SAP与SD - OCT检测青光眼病情进展的能力受疾病阶段的显著影响。我们的结果可能为指导临床医生了解这些检查在整个疾病过程中检测变化的相对效用提供有用信息。