Doll Jacob A, Tang Fengming, Cresci Sharon, Ho P Michael, Maddox Thomas M, Spertus John A, Wang Tracy Y
Duke Clinical Research Institute, Durham, NC Department of Medicine, Duke University, Durham, NC
Saint Luke's Mid America Heart Institute, Kansas City, MO University of Missouri-Kansas City, Kansas City, MO.
J Am Heart Assoc. 2016 Jun 13;5(6):e003205. doi: 10.1161/JAHA.116.003205.
Angina is common both before and after myocardial infarction (MI). Whether the change in angina status within the first 30 days after MI is associated with subsequent readmission and angina persistence is unknown.
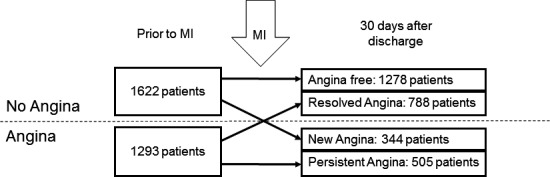
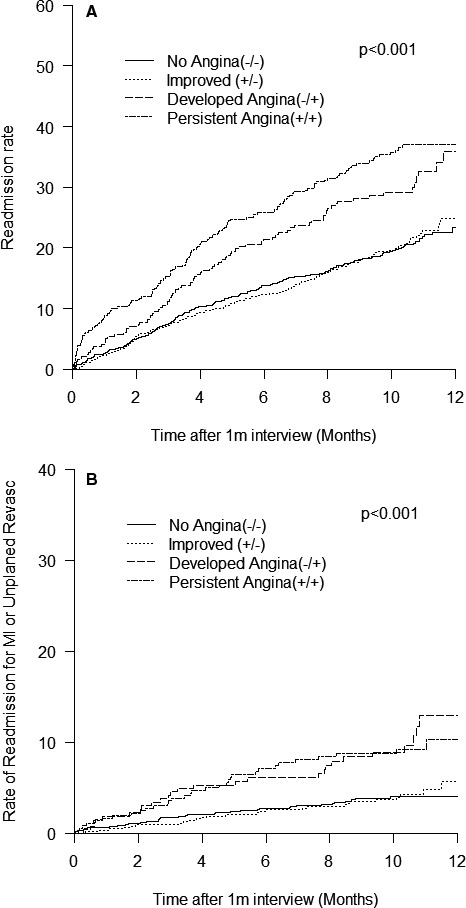
We studied 2915 MI patients enrolled at 24 hospitals in the Translational Research Investigating Underlying Disparities in Acute Myocardial Infarction Patients' Health Status (TRIUMPH) registry. Angina before and 30 days after MI was assessed with the Seattle Angina Questionnaire. Patients were divided into angina-free pre- and post-MI (-/-), resolved angina (+/-), new angina (-/+), and persistent angina (+/+) groups. Multivariable proportional hazards and hierarchical modified Poisson models were performed to assess the association of each group with all-cause readmission, readmission for MI or unplanned revascularization, and angina persistence at 1 year. Overall, 1293 patients (44%) had angina before their MI and 849 (29%) reported angina within 30 days of discharge. Patients with post-MI angina were more likely to be younger, nonwhite, and uninsured. Compared with patients who were angina-free pre- and post-MI, 1-year all-cause readmission risks were significantly higher for patients with persistent angina (hazard ratio [HR], 1.35; 95% CI 1.06-1.71) or new angina (HR, 1.40; 95% CI, 1.08-1.82). At 1 year, angina was present in 22% of patients and was more likely if angina was persistent (HR, 3.55; 95% CI, 3.05-4.13) or new (HR, 3.38; 95% CI, 2.59-4.42) at 30 days compared with patients who were angina-free pre- and post-MI.
Post-MI angina, whether new or persistent, is associated with higher likelihood of readmission. Prioritizing post-MI angina management is a potential means of improving 1-year outcomes.
心绞痛在心肌梗死(MI)前后均很常见。MI后30天内心绞痛状态的变化是否与随后的再入院和心绞痛持续存在相关尚不清楚。
我们研究了参与急性心肌梗死患者健康状况潜在差异转化研究(TRIUMPH)注册研究的24家医院的2915例MI患者。使用西雅图心绞痛问卷评估MI前和MI后30天的心绞痛情况。患者被分为MI前后无心绞痛(-/-)、心绞痛缓解(+/-)、新发心绞痛(-/+)和持续性心绞痛(+/+)组。采用多变量比例风险模型和分层修正泊松模型来评估每组与全因再入院、因MI或计划外血运重建再入院以及1年内心绞痛持续存在之间的关联。总体而言,1293例患者(44%)在MI前有心绞痛,849例(29%)在出院后30天内报告有心绞痛。MI后有心绞痛的患者更可能较年轻、非白人且未参保。与MI前后无心绞痛的患者相比,持续性心绞痛患者(风险比[HR],1.35;95%可信区间[CI] 1.06 - 1.71)或新发心绞痛患者(HR,1.40;95% CI,1.08 - 1.82)的1年全因再入院风险显著更高。在1年时,22%的患者有心绞痛,与MI前后无心绞痛的患者相比,如果在30天时心绞痛为持续性(HR,3.55;95% CI,3.05 - 4.13)或新发(HR,3.38;95% CI,2.59 - 4.42),则心绞痛更可能持续存在。
MI后心绞痛,无论是新发还是持续性,均与再入院可能性较高相关。将MI后心绞痛管理作为优先事项是改善1年结局的一种潜在手段。