Yannopoulos Demetris, Bartos Jason A, Martin Cindy, Raveendran Ganesh, Missov Emil, Conterato Marc, Frascone R J, Trembley Alexander, Sipprell Kevin, John Ranjit, George Stephen, Carlson Kathleen, Brunsvold Melissa E, Garcia Santiago, Aufderheide Tom P
Division of Cardiology, Department of Medicine, University of Minnesota School of Medicine, Minneapolis, MN
Division of Cardiology, Department of Medicine, University of Minnesota School of Medicine, Minneapolis, MN.
J Am Heart Assoc. 2016 Jun 13;5(6):e003732. doi: 10.1161/JAHA.116.003732.
In 2015, the Minnesota Resuscitation Consortium (MRC) implemented an advanced perfusion and reperfusion life support strategy designed to improve outcome for patients with out-of-hospital refractory ventricular fibrillation/ventricular tachycardia (VF/VT). We report the outcomes of the initial 3-month period of operations.
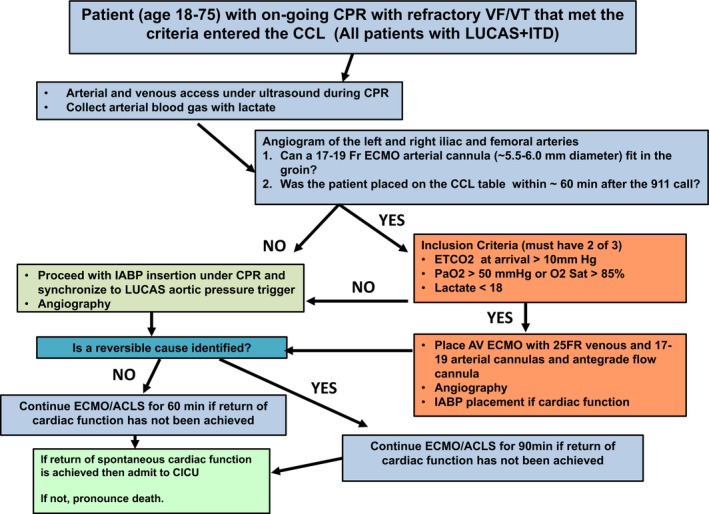
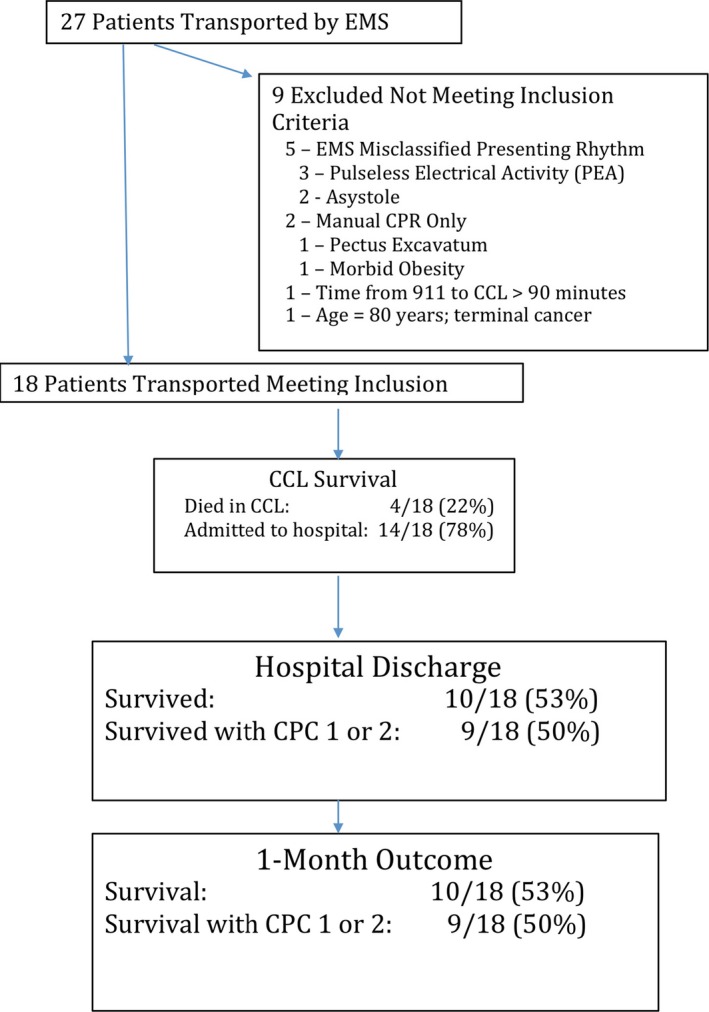
Three emergency medical services systems serving the Minneapolis-St. Paul metro area participated in the protocol. Inclusion criteria included age 18 to 75 years, body habitus accommodating automated Lund University Cardiac Arrest System (LUCAS) cardiopulmonary resuscitation (CPR), and estimated transfer time from the scene to the cardiac catheterization laboratory of ≤30 minutes. Exclusion criteria included known terminal illness, Do Not Resuscitate/Do Not Intubate status, traumatic arrest, and significant bleeding. Refractory VF/VT arrest was defined as failure to achieve sustained return of spontaneous circulation after treatment with 3 direct current shocks and administration of 300 mg of intravenous/intraosseous amiodarone. Patients were transported to the University of Minnesota, where emergent advanced perfusion strategies (extracorporeal membrane oxygenation; ECMO), followed by coronary angiography and primary coronary intervention (PCI), were performed, when appropriate. Over the first 3 months of the protocol, 27 patients were transported with ongoing mechanical CPR. Of these, 18 patients met the inclusion and exclusion criteria. ECMO was placed in 83%. Seventy-eight percent of patients had significant coronary artery disease with a high degree of complexity and 67% received PCI. Seventy-eight percent of patients survived to hospital admission and 55% (10 of 18) survived to hospital discharge, with 50% (9 of 18) achieving good neurological function (cerebral performance categories 1 and 2). No significant ECMO-related complications were encountered.
The MRC refractory VF/VT protocol is feasible and led to a high functionally favorable survival rate with few complications.
2015年,明尼苏达复苏联盟(MRC)实施了一项先进的灌注和再灌注生命支持策略,旨在改善院外难治性室颤/室性心动过速(VF/VT)患者的预后。我们报告了最初3个月的手术结果。
为明尼阿波利斯-圣保罗都会区服务的三个紧急医疗服务系统参与了该方案。纳入标准包括年龄在18至75岁之间、体型适合使用隆德大学自动心脏骤停系统(LUCAS)进行心肺复苏(CPR),以及估计从现场到心脏导管实验室的转运时间≤30分钟。排除标准包括已知的终末期疾病、不进行心肺复苏/不插管状态、创伤性心脏骤停和严重出血。难治性VF/VT心脏骤停定义为在接受3次直流电电击和静脉注射/骨内注射300mg胺碘酮治疗后未能实现持续的自主循环恢复。患者被转运至明尼苏达大学,在适当情况下,进行紧急先进灌注策略(体外膜肺氧合;ECMO),随后进行冠状动脉造影和冠状动脉介入治疗(PCI)。在该方案的前3个月,有27例患者在进行机械CPR的情况下被转运。其中,18例患者符合纳入和排除标准。83%的患者接受了ECMO治疗。78%的患者患有严重的冠状动脉疾病,且病变高度复杂,67%的患者接受了PCI治疗。78%的患者存活至入院,55%(18例中的10例)存活至出院,50%(18例中的9例)获得良好的神经功能(脑功能分级为1级和2级)。未遇到与ECMO相关的严重并发症。
MRC难治性VF/VT方案是可行的,且导致了较高的功能良好生存率,并发症较少。