De Broca Bruno, Garnier Jeremie, Fischer Marc-Olivier, Archange Thomas, Marc Julien, Abou-Arab Osama, Dupont Hervé, Lorne Emmanuel, Guinot Pierre-Grégoire
Anesthesiology and Critical Care Department, Amiens University Medical Center, Place Victor Pauchet, Amiens Pôle Réanimations Anesthésie SAMU/SMUR, CHU de Caen, Caen INSERM U1088, Jules Verne University of Picardy, Amiens, France.
Medicine (Baltimore). 2016 Jul;95(28):e4259. doi: 10.1097/MD.0000000000004259.
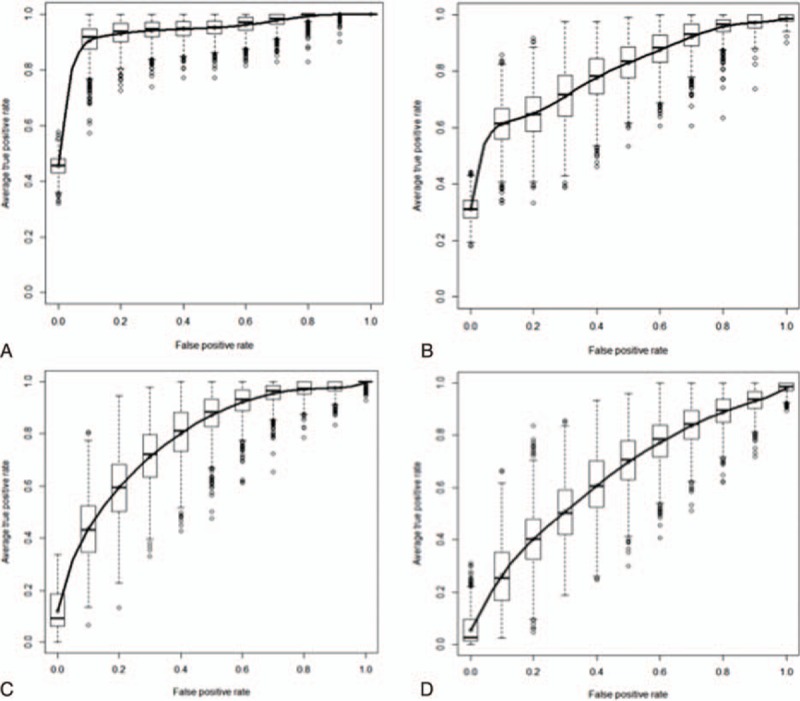
During abdominal surgery, the use of protective ventilation with a low tidal volume, positive expiratory pressure (PEEP) and recruitment maneuvers (RMs) may limit the applicability of dynamic preload indices. The objective of the present study was to establish whether or not the variation in stroke volume (SV) during an RM could predict fluid responsiveness.We prospectively included patients receiving protective ventilation (tidal volume: 6 mL kg, PEEP: 5-7 cmH2O; RMs). Hemodynamic variables, such as heart rate, arterial pressure, SV, cardiac output (CO), respiratory variation in SV (ΔrespSV) and pulse pressure (ΔrespPP), and the variation in SV (ΔrecSV) as well as pulse pressure (ΔrecPP) during an RM were measured at baseline, at the end of the RM, and after fluid expansion. Responders were defined as patients with an SV increase of at least 15% after infusion of 500 mL of crystalloid solution.Thirty-seven (62%) of the 60 included patients were responders. Responders and nonresponders differed significantly in terms of the median ΔrecSV (26% [19-37] vs 10% [4-12], respectively; P < 0.0001). A ΔrecSV value more than 16% predicted fluid responsiveness with an area under the receiver-operating characteristic curve (AU) of 0.95 (95% confidence interval [CI]: 0.91-0.99; P < 0.0001) and a narrow gray zone between 15% and 17%. The area under the curve values for ΔrecPP and ΔrespSV were, respectively, 0.81 (95%CI: 0.7-0.91; P = 0.0001) and 0.80 (95%CI: 0.70-0.94; P < 0.0001). ΔrespPP did not predict fluid responsiveness.During abdominal surgery with protective ventilation, a ΔrecSV value more than 16% accurately predicted fluid responsiveness and had a narrow gray zone (between 15% and 17%). ΔrecPP and ΔrespSV (but not ΔrespPP) were also predictive.
在腹部手术期间,采用低潮气量、呼气末正压(PEEP)和肺复张手法(RM)进行保护性通气可能会限制动态前负荷指标的适用性。本研究的目的是确定RM期间每搏输出量(SV)的变化是否能够预测液体反应性。我们前瞻性纳入了接受保护性通气(潮气量:6 mL/kg,PEEP:5 - 7 cmH₂O;RM)的患者。在基线、RM结束时以及液体扩容后,测量了血流动力学变量,如心率、动脉压、SV、心输出量(CO)、SV的呼吸变化(ΔrespSV)和脉压(ΔrespPP),以及RM期间SV的变化(ΔrecSV)和脉压(ΔrecPP)。反应者定义为输注500 mL晶体液后SV增加至少15%的患者。纳入的60例患者中有37例(62%)为反应者。反应者和非反应者在ΔrecSV中位数方面有显著差异(分别为26% [19 - 37] 与10% [4 - 12];P < 0.0001)。ΔrecSV值大于16%预测液体反应性的受试者工作特征曲线下面积(AU)为0.95(95%置信区间[CI]:0.91 - 0.99;P < 0.0001),在15%至17%之间有一个狭窄的灰色区域。ΔrecPP和ΔrespSV的曲线下面积值分别为0.81(95%CI:0.7 - 0.91;P = 0.0001)和0.80(95%CI:0.70 - 0.94;P < 0.0001)。ΔrespPP不能预测液体反应性。在采用保护性通气的腹部手术期间,ΔrecSV值大于16%能准确预测液体反应性,且有一个狭窄的灰色区域(在15%至17%之间)。ΔrecPP和ΔrespSV(但不是ΔrespPP)也具有预测性。