Laurens Matthew B, Mungwira Randy G, Nyirenda Osward M, Divala Titus H, Kanjala Maxwell, Muwalo Francis, Mkandawire Felix A, Tsirizani Lufina, Nyangulu Wongani, Mwinjiwa Edson, Taylor Terrie E, Mallewa Jane, Blackwelder William C, Plowe Christopher V, Laufer Miriam K, van Oosterhout Joep J
Division of Malaria Research, Institute for Global Health, University of Maryland School of Medicine, 480 W Baltimore St, Room 480, Baltimore, MD, 21218, USA.
Blantyre Malaria Project, Blantyre, Malawi.
Trials. 2016 Jul 18;17(1):322. doi: 10.1186/s13063-016-1392-3.
Before antiretroviral therapy (ART) became widely available in sub-Saharan Africa, several studies demonstrated that daily trimethoprim-sulfamethoxazole (TS) prophylaxis reduced morbidity and mortality among HIV-infected adults. As a result, the World Health Organization (WHO) recommended administering TS prophylaxis to this group. However, the applicability of the results to individuals taking ART and living in sub-Saharan Africa has not been definitively evaluated. This study aims to determine if TS prophylaxis benefits HIV-infected Malawian adults after a good response to ART. If TS prophylaxis does indeed show benefit, it is important to determine if this is due to its antibacterial and/or antimalarial properties.
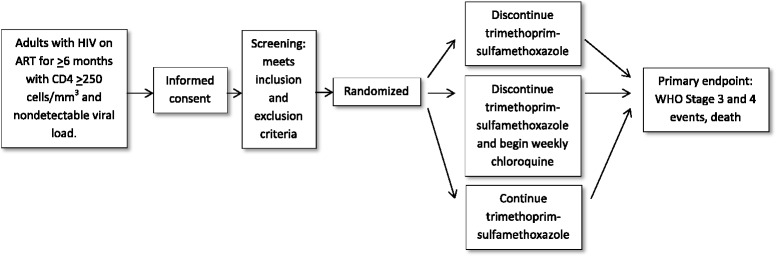
METHODS/DESIGN: A randomized, controlled, open-label, phase III trial of continued standard of care prophylaxis with daily trimethoprim-sulfamethoxazole (TS) compared to discontinuation of standard of care TS prophylaxis and starting weekly chloroquine (CQ) prophylaxis or discontinuation of standard of care TS prophylaxis. The study will randomize 1400-1500 HIV-infected adults (equally divided over the three study arms) with a nondetectable viral load and a CD4 count of 250/mm(3) or more from antiretroviral therapy clinics in Blantyre and Zomba. The expected rate of primary endpoint events of death and WHO stage 3 and 4 events is 6.8 per 100 person-years of follow-up in all participants. Assuming the number of events follows a Poisson distribution and average participant follow-up after 10 % loss to follow-up is 41.6 months, the study will have approximately 85 % power to rule out a reduction of 35 % or more in primary endpoint events in the TS or CQ arms compared to discontinuation of TS prophylaxis-i.e., to show that discontinuation of TS prophylaxis is noninferior to either TS or CQ, with a noninferiority margin of 35 %. Ethical and regulatory approvals were obtained from the University of Malawi College of Medicine Research Ethics Committee; the Malawi Pharmacy, Medicines and Poisons Board; and the University of Maryland Baltimore Institutional Review Board.
The study began recruitment activities at the Ndirande site in November 2012. The sponsor agreed to extend and expand the study in early 2015, and a second site, Zomba, was added for recruitment and follow-up in mid-2015.
ClinicalTrials.gov Identifier: NCT01650558 (registered on 6 July 2012).
Letter of amendment #1 to the DAIDS-ES 10822 TSCQ Malawi Protocol, Version 4.0, 16 December 2014.
在抗逆转录病毒疗法(ART)在撒哈拉以南非洲广泛应用之前,多项研究表明,每日服用甲氧苄啶 - 磺胺甲恶唑(TS)进行预防可降低HIV感染成人的发病率和死亡率。因此,世界卫生组织(WHO)建议对该群体进行TS预防治疗。然而,这些结果对于在撒哈拉以南非洲接受ART治疗的个体的适用性尚未得到明确评估。本研究旨在确定在对ART有良好反应后,TS预防对感染HIV的马拉维成人是否有益。如果TS预防确实显示出益处,确定这是否归因于其抗菌和/或抗疟特性很重要。
方法/设计:一项随机、对照、开放标签的III期试验,将继续每日服用甲氧苄啶 - 磺胺甲恶唑(TS)进行标准护理预防,与停止标准护理TS预防并开始每周服用氯喹(CQ)预防或停止标准护理TS预防进行比较。该研究将从布兰太尔和宗巴的抗逆转录病毒治疗诊所中随机选取1400 - 1500名HIV感染成人(平均分配到三个研究组),这些成人病毒载量不可检测,且CD4细胞计数为每立方毫米250个或更多。所有参与者中,主要终点事件(死亡以及WHO 3期和4期事件)的预期发生率为每100人年随访6.8例。假设事件数服从泊松分布,在10%失访后平均参与者随访时间为41.6个月,该研究将有大约85%的把握排除TS或CQ组与停止TS预防组相比主要终点事件减少35%或更多的情况,即表明停止TS预防不劣于TS或CQ,非劣效界值为35%。已获得马拉维大学医学院研究伦理委员会、马拉维药房、药品和毒物委员会以及马里兰大学巴尔的摩分校机构审查委员会的伦理和监管批准。
该研究于2012年11月在恩迪兰德站点开始招募活动。资助者于2015年初同意扩展和扩大该研究,并于2015年年中增加了第二个站点宗巴进行招募和随访。
ClinicalTrials.gov标识符:NCT01650558(于2012年7月6日注册)。
2014年1December 16日对DAIDS - ES 10822 TSCQ马拉维方案第4.0版的修订信#1。