Department of Urology, Kyungpook National University School of Medicine, Daegu, Korea.
Investig Clin Urol. 2016 Jul;57(4):260-7. doi: 10.4111/icu.2016.57.4.260. Epub 2016 Jul 6.
The aim of this study was to assess the advantages of robotic surgery, comparing perioperative and oncological outcomes between robot-assisted radical cystectomy (RARC) and open radical cystectomy (ORC).
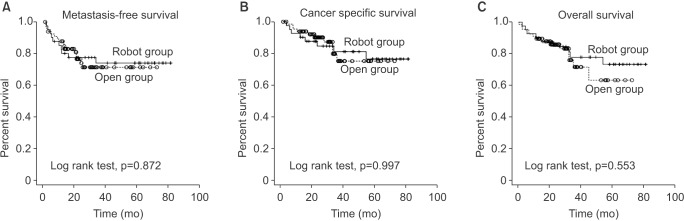
Between August 2008 and May 2014, 112 radical cystectomies (42 RARCs and 70 ORCs) were performed at a single academic institution following Institutional Review Board approval. Patient demographics, perioperative variables (e.g., complications), and oncologic outcomes including metastasis-free survival (MFS), cancer-specific survival (CSS), and overall survival (OS) were reported using the Kaplan-Meier analyses.
The median follow-up period was 40 months (range, 0-70 months) vs. 42 months (range, 0-74 months) in RARC and ORC, respectively. Baseline characteristics of both groups were balanced. Blood loss (median, [range]; 300 mL [125-925 mL] vs. 598 mL [150-2,000 mL], p=0.001) and perioperative transfusion rates (23.8% vs. 45.7%, p=0.020) were significantly lower in the RARC group than in the ORC group. The overall complication rates were greater in the ORC group, but this was not statistically significant (65.7% vs. 64.3%, p=0.878). However, there were significantly higher major complication rates in the ORC group (45.7% vs. 26.2%, p=0.040). No significant differences were found with regards to MFS, CSS, and OS.
While histopathological findings, overall complications, and survival rates do not reveal definite differences, RARC has more advantages compared to ORC in terms of estimated blood loss, perioperative transfusion rates and fewer perioperative major complications. We propose that RARC is a safer treatment modality with equivalent oncological outcomes compared to ORC.
本研究旨在评估机器人手术的优势,比较机器人辅助根治性膀胱切除术(RARC)与开放性根治性膀胱切除术(ORC)的围手术期和肿瘤学结果。
在机构审查委员会批准后,于 2008 年 8 月至 2014 年 5 月,在一家学术机构对 112 例根治性膀胱切除术(42 例 RARC 和 70 例 ORC)进行了回顾性分析。使用 Kaplan-Meier 分析报告患者人口统计学数据、围手术期变量(如并发症)和肿瘤学结果,包括无转移生存率(MFS)、癌症特异性生存率(CSS)和总生存率(OS)。
RARC 和 ORC 的中位随访时间分别为 40 个月(范围,0-70 个月)和 42 个月(范围,0-74 个月)。两组的基线特征平衡。RARC 组的术中出血量(中位数,[范围];300mL[125-925mL] vs. 598mL[150-2000mL],p=0.001)和围手术期输血率(23.8% vs. 45.7%,p=0.020)明显低于 ORC 组。ORC 组的总体并发症发生率较高,但无统计学意义(65.7% vs. 64.3%,p=0.878)。然而,ORC 组的主要并发症发生率明显较高(45.7% vs. 26.2%,p=0.040)。在 MFS、CSS 和 OS 方面无显著差异。
虽然组织病理学发现、总体并发症和生存率没有显示出明确的差异,但 RARC 在估计出血量、围手术期输血率和减少围手术期主要并发症方面与 ORC 相比具有更多优势。我们认为,与 ORC 相比,RARC 是一种更安全的治疗方式,具有等效的肿瘤学结果。