Jiang Yanfang, Sanchez-Santos Maria T, Judge Andrew D, Murray David W, Arden Nigel K
Institute of Sports Medicine, Peking University 3rd Hospital, Beijing, China.
Arthritis Research UK Sports, Exercise and Osteoarthritis Centre of Excellence, University of Oxford, UK; NIHR Musculoskeletal Biomedical Research Unit, Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Oxford, UK.
J Arthroplasty. 2017 Jan;32(1):92-100.e2. doi: 10.1016/j.arth.2016.06.009. Epub 2016 Jun 23.
This study aimed at identifying preoperative predictors of patient-reported outcomes after total knee arthroplasty (TKA) and at investigating their association with the outcomes over time.
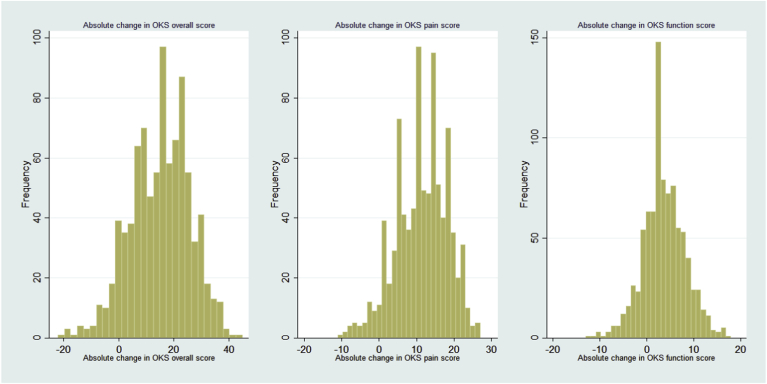
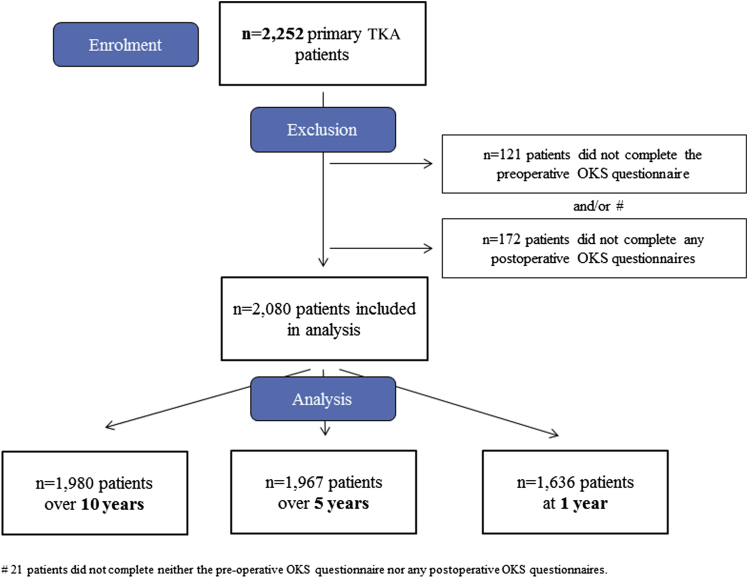
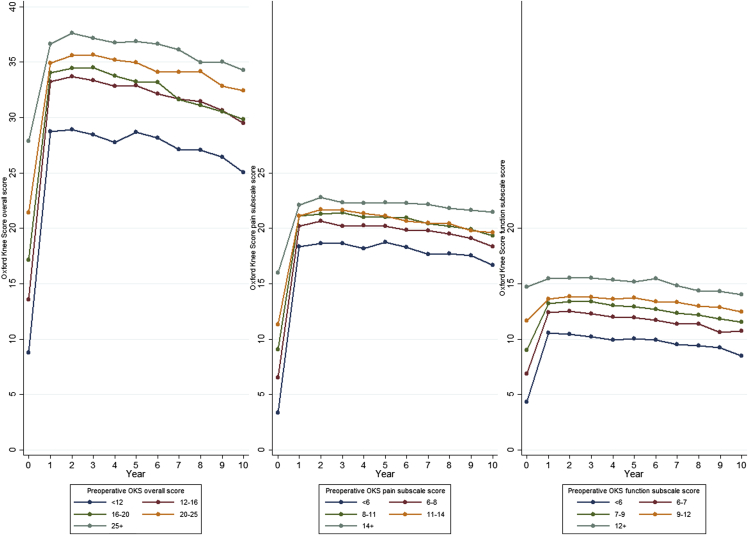
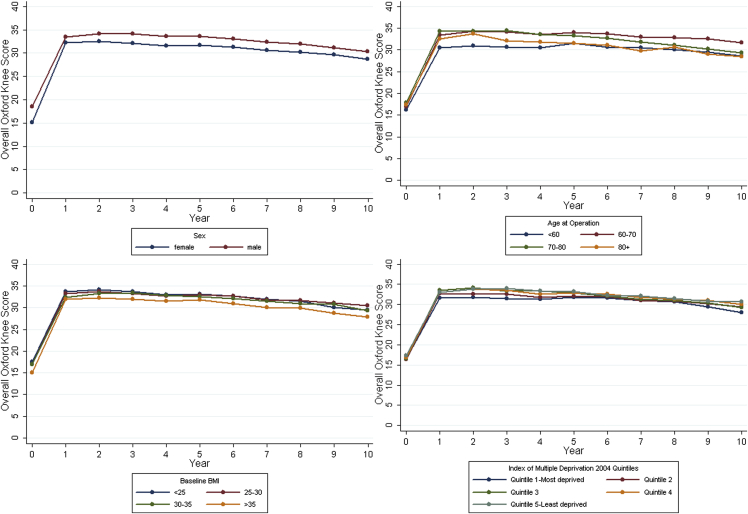
We used data from 2080 patients from the Knee Arthroplasty Trial who received primary TKA in the United Kingdom between July 1999 and January 2003. The primary outcome measure was the Oxford knee score (OKS) collected annually over 10 years after TKA. Preoperative predictors included a range of patient characteristics and clinical conditions. Mixed-effects linear regression model analysis of repeated measurements was used to identify predictors of overall OKS, and pain and function subscale scores over 10 years, separately.
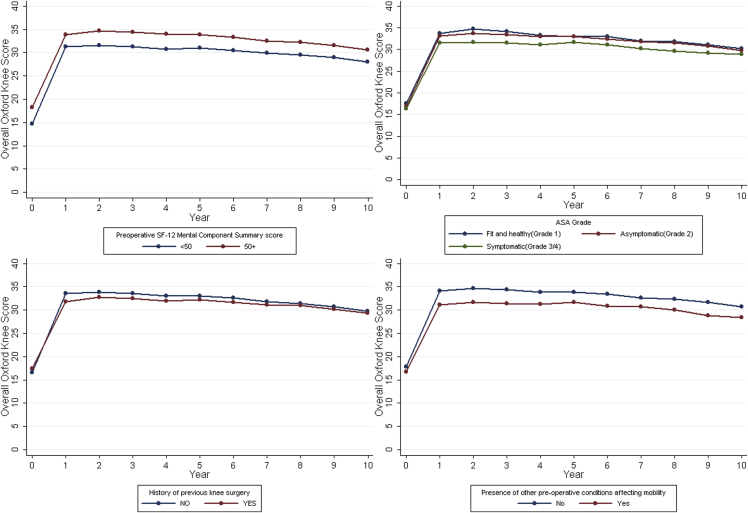
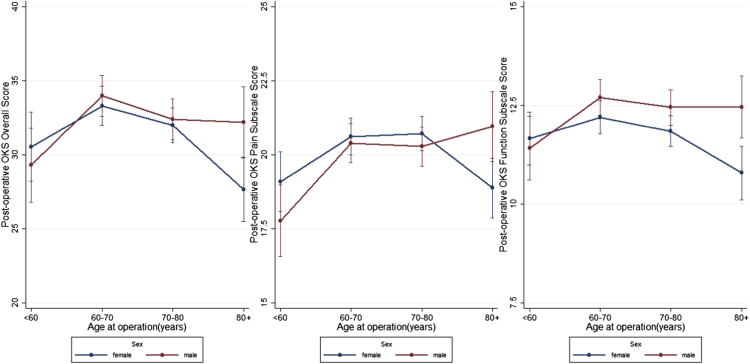
Worse preoperative OKS, worse mental well-being, body mass index greater than 35 kg/m, living in the most deprived areas, higher American Society of Anesthesiologists grade, presence of comorbidities, and history of previous knee surgery were associated with worse overall OKS over 10 years after surgery. The same predictors were identified for pain and function subscale scores, and for both long-term (10 years) and short-to-medium-term outcomes (1 and 5 years). However, fitted models explained more variations in function and shorter-term outcomes than in pain and longer-term outcomes, respectively.
The same predictors were identified for pain and functional outcomes over both short-to-medium term and long term after TKA. Within the factors identified, functional and shorter-term outcomes were more predictable than pain and longer-term outcomes, respectively. Regardless of their preoperative characteristics, on average, patients achieved substantial improvement in pain over time, although improvement for function was less prominent.
本研究旨在确定全膝关节置换术(TKA)后患者报告结局的术前预测因素,并调查它们随时间与结局的关联。
我们使用了来自膝关节置换术试验的2080例患者的数据,这些患者于1999年7月至2003年1月在英国接受了初次TKA。主要结局指标是TKA后10年内每年收集的牛津膝关节评分(OKS)。术前预测因素包括一系列患者特征和临床状况。采用重复测量的混合效应线性回归模型分析来分别确定10年内总体OKS、疼痛和功能子量表评分的预测因素。
术前OKS较差、心理健康状况较差、体重指数大于35 kg/m²、生活在最贫困地区、美国麻醉医师协会分级较高、存在合并症以及既往有膝关节手术史与术后10年内总体OKS较差相关。疼痛和功能子量表评分以及长期(10年)和短期至中期结局(1年和5年)均确定了相同的预测因素。然而,拟合模型分别解释了功能和短期结局的变异比疼痛和长期结局更多。
TKA后短期至中期和长期的疼痛和功能结局确定了相同的预测因素。在确定的因素中,功能和短期结局分别比疼痛和长期结局更具可预测性。无论术前特征如何,随着时间的推移,患者的疼痛平均有显著改善,尽管功能改善不太明显。