McClune Jason R, Wilshire Candice L, Gorden Jed A, Louie Brian E, Farviar Alexander S, Stefanski Michael J, Vallieres Eric, Aye Ralph W, Gilbert Christopher R
Division of Pulmonary, Allergy, and Critical Care Medicine, Penn State Milton S. Hershey Medical Center, Hershey, PA 17033, USA.
Division of Thoracic Surgery and Interventional Pulmonology, Swedish Cancer Institute and Medical Center, Seattle, WA 98104, USA.
Can Respir J. 2016;2016:9796768. doi: 10.1155/2016/9796768. Epub 2016 Jun 30.
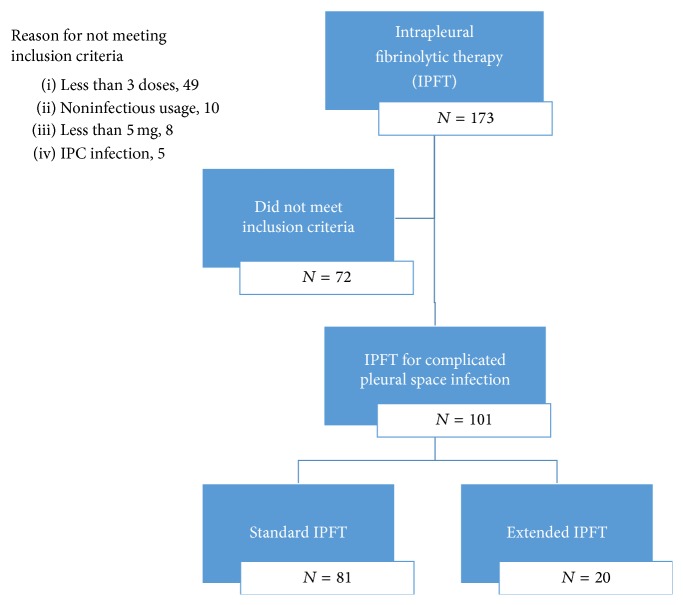
The use of intrapleural therapy with tissue plasminogen activator and DNase improves outcomes in patients with complicated pleural space infections. However, little data exists for the use of combination intrapleural therapy after the initial dosing period of six doses. We sought to describe the safety profile and outcomes of intrapleural therapy beyond this standard dosing. A retrospective review of patients receiving intrapleural therapy with tissue plasminogen activator and DNase was performed at two institutions. We identified 101 patients from January 2013 to August 2015 receiving intrapleural therapy for complicated pleural space infection. The extended use of intrapleural tissue plasminogen activator and DNase therapy beyond six doses was utilized in 20% (20/101) of patients. The mean number of doses in those undergoing extended dosing was 9.8 (range of 7-16). Within the population studied there appears to be no statistically significant increased risk of complications, need for surgical referral, or outcome differences when comparing those receiving standard or extended dosing intrapleural therapy. Future prospective study of intrapleural therapy as an alternative option for patients who fail initial pleural drainage and are unable to tolerate/accept a surgical intervention appears a potential area of study.
使用组织型纤溶酶原激活剂和脱氧核糖核酸酶进行胸膜内治疗可改善复杂性胸膜腔感染患者的预后。然而,在初始六剂给药期之后使用胸膜内联合治疗的数据很少。我们试图描述超出该标准给药的胸膜内治疗的安全性和预后。在两家机构对接受组织型纤溶酶原激活剂和脱氧核糖核酸酶胸膜内治疗的患者进行了回顾性研究。我们确定了2013年1月至2015年8月期间101例因复杂性胸膜腔感染接受胸膜内治疗的患者。20%(20/101)的患者使用了超出六剂的胸膜内组织型纤溶酶原激活剂和脱氧核糖核酸酶延长治疗。延长给药患者的平均给药次数为9.8次(范围为7 - 16次)。在研究人群中,比较接受标准或延长给药胸膜内治疗的患者时,并发症风险、手术转诊需求或预后差异似乎没有统计学上的显著增加。对于初始胸腔引流失败且无法耐受/接受手术干预的患者,胸膜内治疗作为一种替代选择的未来前瞻性研究似乎是一个潜在的研究领域。