Fanari Zaher, Malodiya Amratash, Weiss Sandra A, Hammami Sumaya, Kolm Paul, Weintraub William S
University of Kansas School of Medicine, Kansas City, KS; Section of Cardiology, Christiana Care Health System, Newark, DE.
Section of Cardiology, Christiana Care Health System, Newark, DE.
Cardiovasc Revasc Med. 2017 Jan-Feb;18(1):10-15. doi: 10.1016/j.carrev.2016.07.006. Epub 2016 Jul 20.
The potential benefit of long-term dual antiplatelet therapy (DAPT) for secondary prevention of atherothrombotic events is unclear. Data from different randomized controlled trials (RCT) using different agents in different subgroups showed inconsistent results.
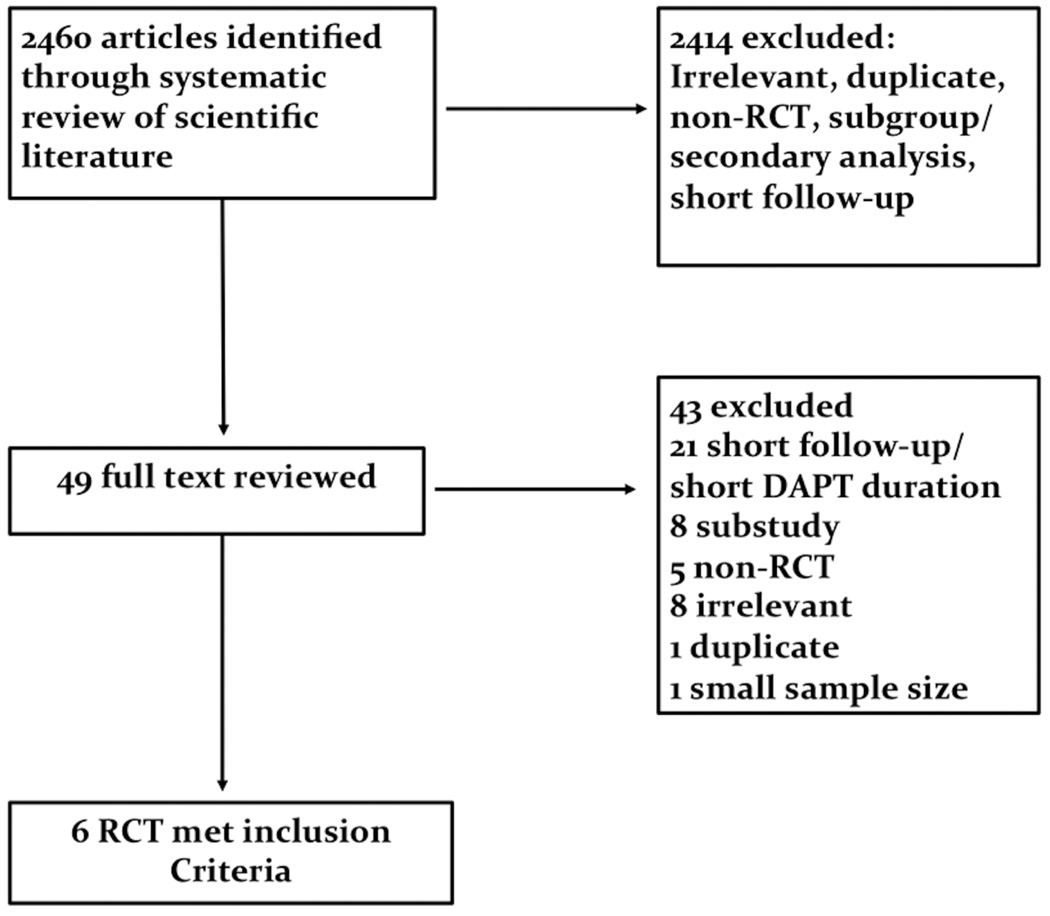
We performed a systematic review and meta-analysis from RCTs that tested different prolonged durations of DAPT for secondary prevention. Long term DAPT arm was defined as those receiving DAPT for more than 12months. Long-term aspirin arm was defined as those receiving either aspirin alone long term or DAPT for less than 12months.
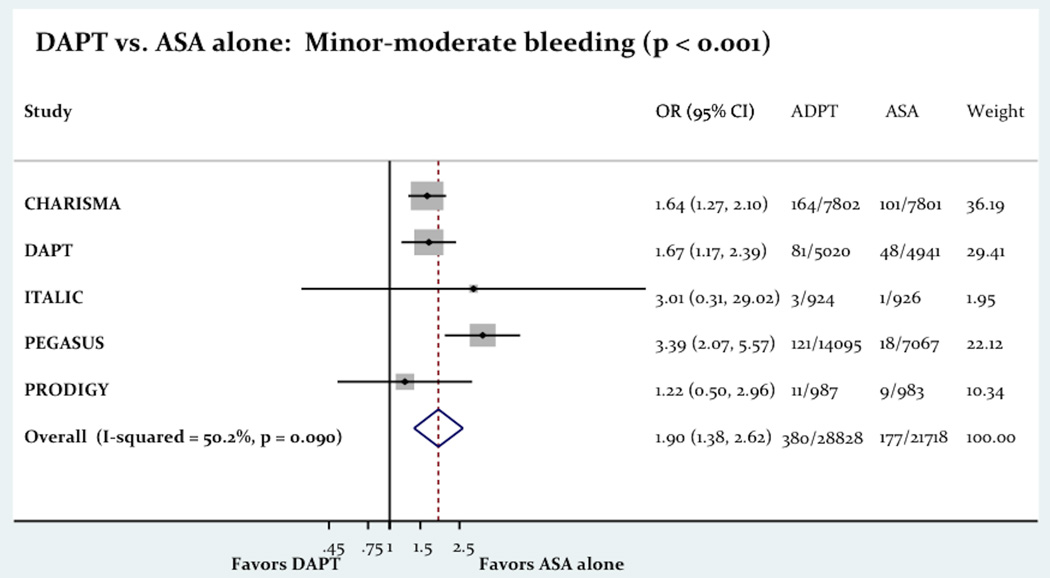
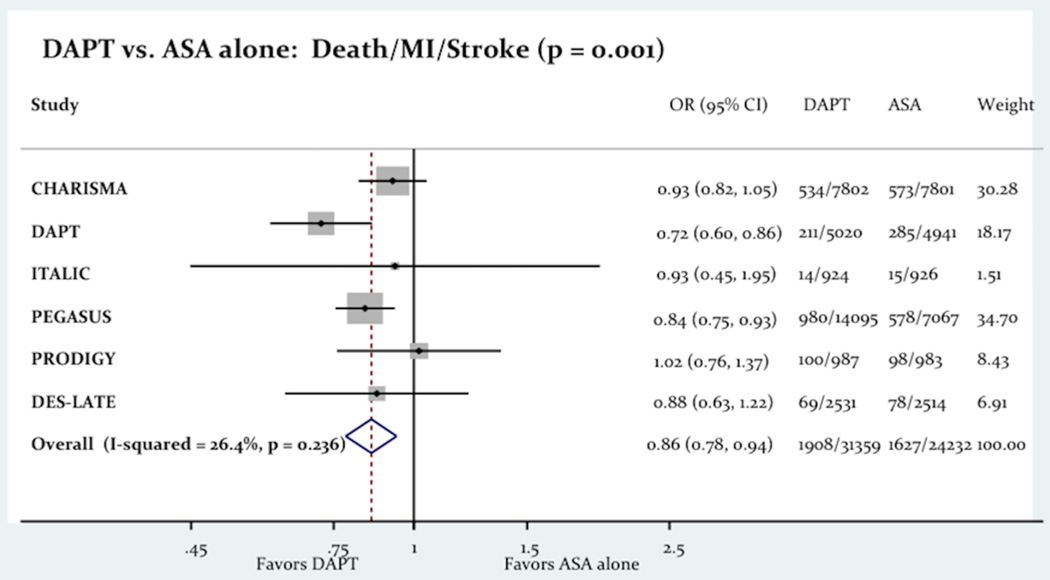
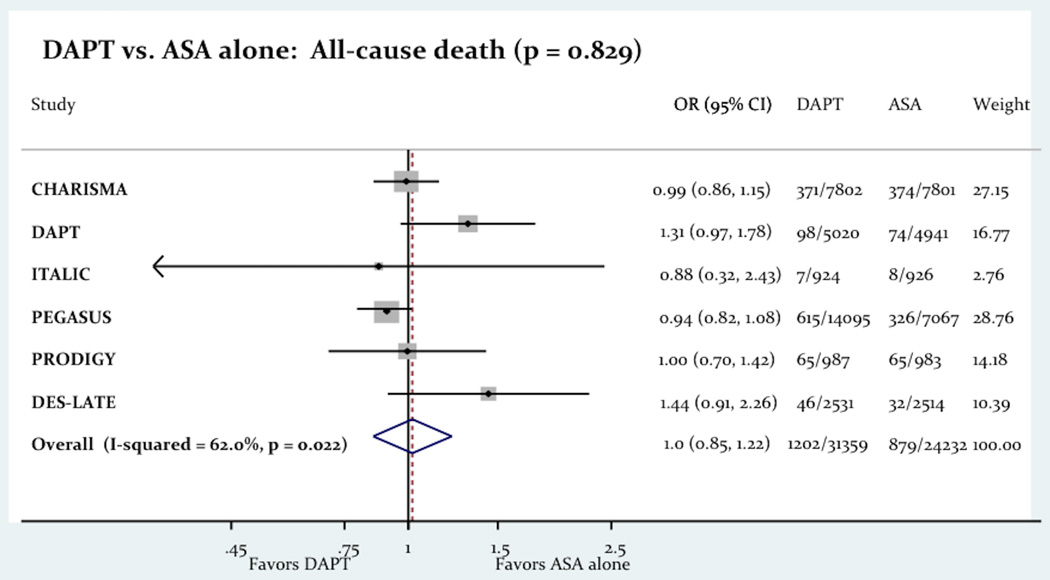
The use of long term DAPT was associated with a significant decrease in composite of death, myocardial infarction (MI) and stroke (6.08% vs. 6.71%; odds ratio OR=0.86 [0.78-0.94]; P=0.001). This reduction of death, MI and stroke was mainly noticed in patients with prior MI or stroke, but not with PAD or multiple risk factors. The reduction was seen with post PCI patients with prasugrel and only in those with prior MI with clopidogrel and ticagrelor. Long-term use of DAPT was associated with significant increase in major bleeding (1.47% vs. 0.88%; OR=1.65 [1.23-2.21]; P=0.001).
Long-term use of DAPT for secondary prevention is associated with lower risk of death, MI and stroke beneficial especially in patients with prior MI and stroke, but it is associated with increased risk of bleeding. Prolonging DAPT requires careful assessment of the trade-off between ischemic and bleeding complications and should probably be reserved for patients with higher risk for atherothrombotic events.
长期双联抗血小板治疗(DAPT)用于动脉粥样硬化血栓形成事件二级预防的潜在益处尚不清楚。来自不同随机对照试验(RCT)的数据,在不同亚组中使用不同药物,结果并不一致。
我们对测试不同延长疗程DAPT用于二级预防的RCT进行了系统评价和荟萃分析。长期DAPT组定义为接受DAPT超过12个月的患者。长期阿司匹林组定义为长期单独接受阿司匹林治疗或接受DAPT少于12个月的患者。
长期使用DAPT与死亡、心肌梗死(MI)和卒中的复合终点显著降低相关(6.08%对6.71%;优势比OR = 0.86 [0.78 - 0.94];P = 0.001)。死亡、MI和卒中的这种降低主要见于既往有MI或卒中的患者,而PAD或多种危险因素患者未见此降低。PCI术后使用普拉格雷的患者以及既往有MI使用氯吡格雷和替格瑞洛的患者中可见此降低。长期使用DAPT与严重出血显著增加相关(1.47%对0.88%;OR = 1.65 [1.23 - 2.21];P = 0.001)。
长期使用DAPT进行二级预防与死亡、MI和卒中风险降低相关,尤其对既往有MI和卒中的患者有益,但与出血风险增加相关。延长DAPT疗程需要仔细评估缺血和出血并发症之间的权衡,可能应仅用于动脉粥样硬化血栓形成事件风险较高的患者。