Singh Samiksha, Doyle Pat, Campbell Oona M, Mathew Manu, Murthy G V S
Indian Institute of Public Health-Hyderabad, Public Health Foundation of India, Hyderabad, Telangana, India.
Department of Non-communicable disease Epidemiology, Faculty of EPH, London School of Hygiene and Tropical Medicine, London, United Kingdom.
PLoS One. 2016 Aug 3;11(8):e0159793. doi: 10.1371/journal.pone.0159793. eCollection 2016.
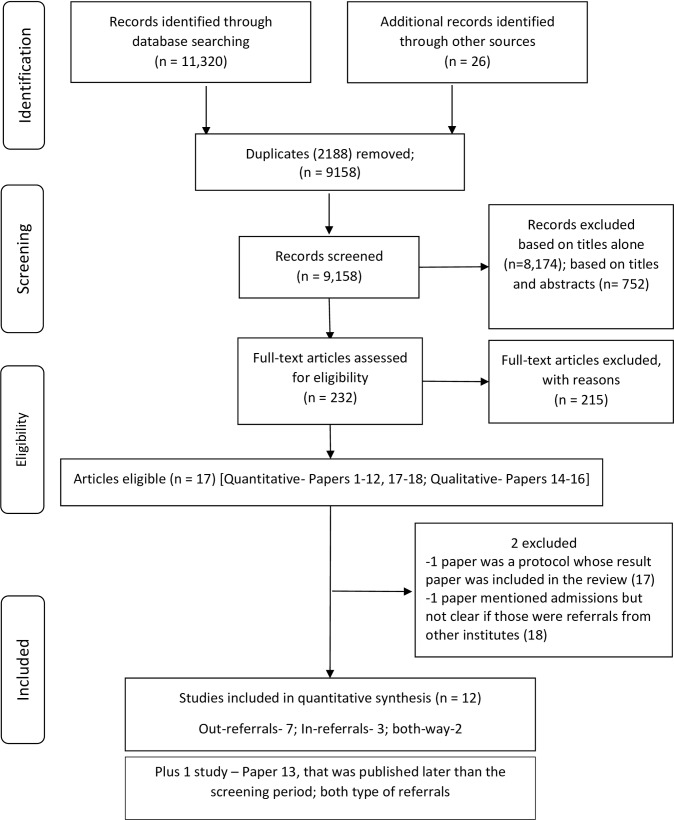
Emergency obstetric care (EmOC) within primary health care systems requires a linked referral system to be effective in reducing maternal death. This systematic review aimed to summarize evidence on the proportion of referrals between institutions during pregnancy and delivery, and the factors affecting referrals, in India. We searched 6 electronic databases, reviewed four regional databases and repositories, and relevant program reports from India published between 1994 and 2013. All types of study or reports (except editorials, comments and letters) which reported on institution-referrals (out-referral or in-referral) for obstetric care were included. Results were synthesized on the proportion and the reasons for referral, and factors affecting referrals. Of the 11,346 articles identified by the search, we included 232 articles in the full text review and extracted data from 16 studies that met our inclusion criteria Of the 16, one was RCT, seven intervention cohort (without controls), six cross-sectional, and three qualitative studies. Bias and quality of studies were reported. Between 25% and 52% of all pregnancies were referred from Sub-centres for antenatal high-risk, 14% to 36% from nurse run delivery or basic EmOC centres for complications or emergencies, and 2 to 7% were referred from doctor run basic EmOC centres for specialist care at comprehensive EmOC centres. Problems identified with referrals from peripheral health centres included low skills and confidence of staff, reluctance to induce labour, confusion over the clinical criteria for referral, non-uniform standards of care at referral institutions, a tendency to by-pass middle level institutions, a lack of referral communication and supervision, and poor compliance. The high proportion of referrals from peripheral health centers reflects the lack of appropriate clinical guidelines, processes, and skills for obstetric care and referral in India. This, combined with inadequate referral communication and low compliance, is likely to contribute to gaps and delays in the provision of emergency obstetric care.
初级卫生保健系统中的紧急产科护理(EmOC)需要一个有效的转诊系统来降低孕产妇死亡率。本系统评价旨在总结印度孕期和分娩期间机构间转诊比例以及影响转诊因素的证据。我们检索了6个电子数据库,查阅了4个区域数据库和知识库,以及1994年至2013年期间印度发布的相关项目报告。纳入所有报告产科护理机构转诊(转出或转入)情况的各类研究或报告(社论、评论和信件除外)。综合分析了转诊比例、原因及影响因素。在检索到的11346篇文章中,我们纳入232篇进行全文综述,并从16项符合纳入标准的研究中提取数据。这16项研究中,1项为随机对照试验,7项为干预队列研究(无对照),6项为横断面研究,3项为定性研究。报告了研究的偏倚和质量。所有妊娠中,25%至52%从分中心转诊至产前高危机构,14%至36%从护士接生或基本EmOC中心转诊至处理并发症或紧急情况的机构,2%至7%从医生主导的基本EmOC中心转诊至综合EmOC中心接受专科护理。从基层卫生中心转诊存在的问题包括工作人员技能和信心不足、不愿引产、转诊临床标准不明确、转诊机构护理标准不统一、绕过中级机构的倾向、缺乏转诊沟通和监督以及依从性差。基层卫生中心转诊比例高反映出印度产科护理和转诊缺乏适当的临床指南、流程和技能。这与转诊沟通不足和依从性低相结合,可能导致紧急产科护理出现差距和延误。