Magill Department of Anaesthesia, Intensive Care Medicine and Pain Management, Chelsea and Westminster Hospital, London, UK.
Burns Trauma. 2014 Jan 26;2(1):29-35. doi: 10.4103/2321-3868.126090. eCollection 2014.
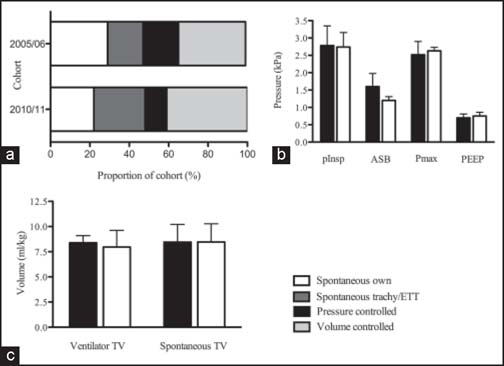
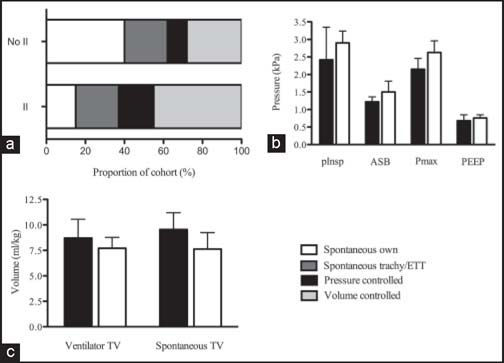
Consensus regarding optimal burns intensive care (BICU) patient management is lacking. This study aimed to assess whether ventilation strategies, cardiovascular support and sedation in BICU patients have changed over time, and whether this affects outcome. A retrospective observational study comparing two 12-patient BICU cohorts (2005/06 and 2010/11) was undertaken. Demographic and admission characteristics, ventilation parameters, sedation, fluid resuscitation, cardiovascular support and outcome (length of stay, mortality) data were collected from patient notes. Data was analysed using T-tests, Fisher's exact and Mann-Whitney U tests. In our study cohort groups were equivalent in demographic and admission parameters. There were equal ventilator-free days in the two cohorts 10 ± 12.7 vs. 13.3 ± 12.2 ventilator free days; P = 0.447). The 2005/06 cohort were mechanically ventilated more often than in 2010/11 cohort (568 ventilator days/1000 patient BICU days vs. 206 ventilator days/1000 patient BICU days; P = 0.001). The 2005/06 cohort were ventilated less commonly in tracheostomy group/endotracheal tube spontaneous (17.8% vs. 26%; P = 0.001) and volume-controlled modes (34.4% vs. 40.8%; P = 0.001). Patients in 2010/11 cohort were more heavily sedated (P = 0.001) with more long-acting sedative drug use (P = 0.001) than the 2005/06 cohort, fluid administration was equivalent. Patient outcome did not vary. Inhalational injury patients were ventilated in volume-controlled (44.5% vs. 28.1%; P = 0.001) and pressure-controlled modes (18.2% vs. 9.5%; P = 0.001) more frequently than those without. Outcome did not vary. This study showed there has been shift away from mechanical ventilation, with increased use of tracheostomy/tracheal tube airway spontaneous ventilation. Inhalation injury patients require more ventilatory support though patient outcomes do not differ. Prospective trials are required to establish which strategies confer benefit.
关于烧伤重症监护(BICU)患者最佳管理的共识尚缺乏。本研究旨在评估 BICU 患者的通气策略、心血管支持和镇静是否随时间发生了变化,以及这是否会影响结果。我们进行了一项回顾性观察性研究,比较了两个 12 名 BICU 患者队列(2005/06 年和 2010/11 年)。从患者病历中收集人口统计学和入院特征、通气参数、镇静、液体复苏、心血管支持和结局(住院时间、死亡率)数据。使用 T 检验、Fisher 确切检验和 Mann-Whitney U 检验进行数据分析。在我们的研究队列中,两组在人口统计学和入院参数方面是等效的。两组的无呼吸机天数相等,分别为 10 ± 12.7 天和 13.3 ± 12.2 天;P = 0.447)。2005/06 年队列的机械通气频率高于 2010/11 年队列(568 个呼吸机日/1000 个患者 BICU 日比 206 个呼吸机日/1000 个患者 BICU 日;P = 0.001)。2005/06 年队列在气管切开术组/气管内管自主通气(17.8%比 26%;P = 0.001)和容量控制模式(34.4%比 40.8%;P = 0.001)中通气的频率较低。2010/11 年队列的患者镇静程度更高(P = 0.001),使用长效镇静药物的频率更高(P = 0.001),而 2005/06 年队列的患者镇静程度更高,液体管理则相同。患者的预后没有差异。吸入性损伤患者在容量控制(44.5%比 28.1%;P = 0.001)和压力控制(18.2%比 9.5%;P = 0.001)模式下通气的频率高于没有吸入性损伤的患者。但预后没有差异。本研究表明,机械通气的使用减少,气管切开术/气管内管自主通气的使用增加。尽管吸入性损伤患者需要更多的通气支持,但患者的预后没有差异。需要进行前瞻性试验来确定哪些策略有益。