Upadhyay Ushma D, Johns Nicole E, Combellick Sarah L, Kohn Julia E, Keder Lisa M, Roberts Sarah C M
Advancing New Standards in Reproductive Health (ANSIRH), Bixby Center for Global Reproductive Health, Department of Obstetrics, Gynecology and Reproductive Sciences, University of California, San Francisco, Oakland, California, United States of America.
Planned Parenthood Federation of America, New York, New York, United States of America.
PLoS Med. 2016 Aug 30;13(8):e1002110. doi: 10.1371/journal.pmed.1002110. eCollection 2016 Aug.
In February 2011, an Ohio law took effect mandating use of the United States Food and Drug Administration (FDA)-approved protocol for mifepristone, which is used with misoprostol for medication abortion. Other state legislatures have passed or enacted similar laws requiring use of the FDA-approved protocol for medication abortion. The objective of this study is to examine the association of this legal change with medication abortion outcomes and utilization.
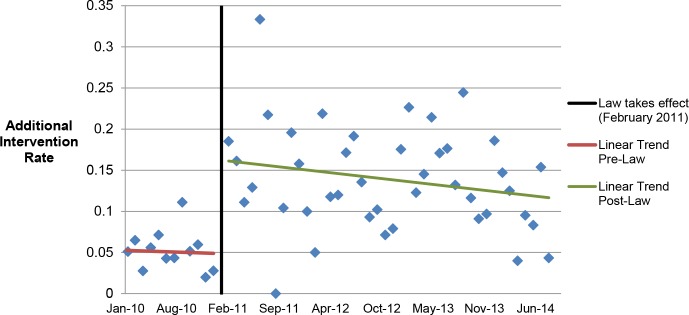
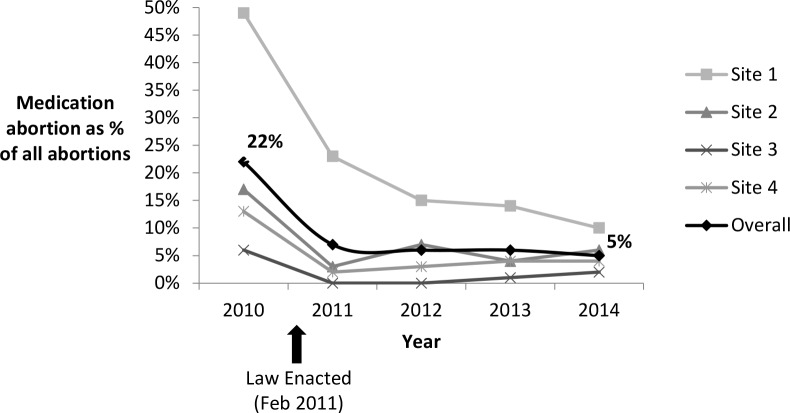
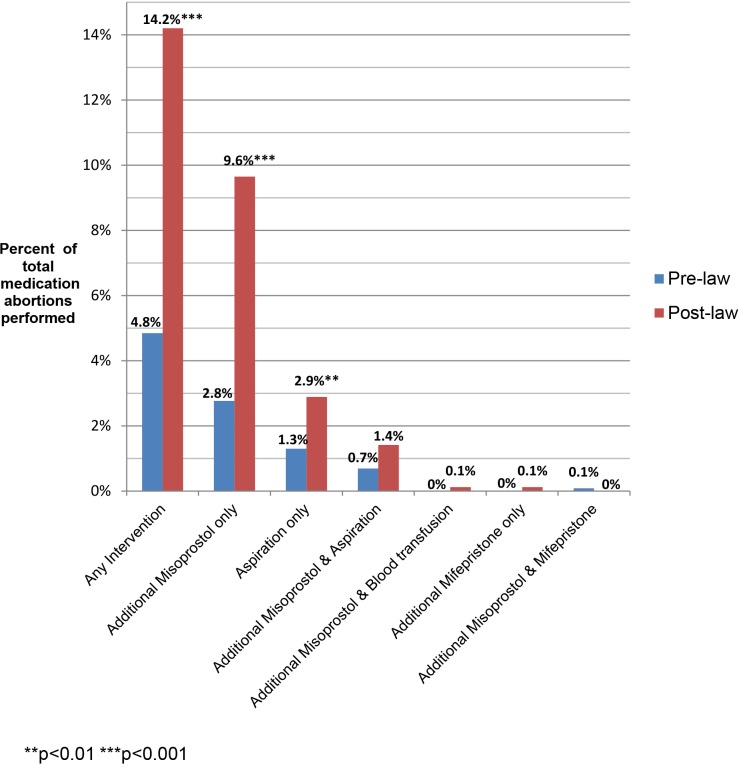
We used a retrospective cohort design, comparing outcomes of medication abortion patients in the prelaw period to those in the postlaw period. Sociodemographic and clinical chart data were abstracted from all medication abortion patients from 1 y prior to the law's implementation (January 2010-January 2011) to 3 y post implementation (February 2011-October 2014) at four abortion-providing health care facilities in Ohio. Outcome data were analyzed for all women undergoing abortion at ≤49 d gestation during the study period. The main outcomes were as follows: need for additional intervention following medication abortion (such as aspiration, repeat misoprostol, and blood transfusion), frequency of continuing pregnancy, reports of side effects, and the proportion of abortions that were medication abortions (versus other abortion procedures). Among the 2,783 medication abortions ≤49 d gestation, 4.9% (95% CI: 3.7%-6.2%) in the prelaw and 14.3% (95% CI: 12.6%-16.0%) in the postlaw period required one or more additional interventions. Women obtaining a medication abortion in the postlaw period had three times the odds of requiring an additional intervention as women in the prelaw period (adjusted odds ratio [AOR] = 3.11, 95% CI: 2.27-4.27). In a mixed effects multivariable model that uses facility-months as the unit of analysis to account for lack of independence by site, we found that the law change was associated with a 9.4% (95% CI: 4.0%-18.4%) absolute increase in the rate of requiring an additional intervention. The most common subsequent intervention in both periods was an additional misoprostol dose and was most commonly administered to treat incomplete abortion. The percentage of women requiring two or more follow-up visits increased from 4.2% (95% CI: 3.0%-5.3%) in the prelaw period to 6.2% (95% CI: 5.5%-8.0%) in the postlaw period (p = 0.003). Continuing pregnancy was rare (0.3%). Overall, 12.6% of women reported at least one side effect during their medication abortion: 8.4% (95% CI: 6.8%-10.0%) in the prelaw period and 15.6% (95% CI: 13.8%-17.3%) in the postlaw period (p < 0.001). Medication abortions fell from 22% (95% CI: 20.8%-22.3%) of all abortions the year before the law went into effect (2010) to 5% (95% CI: 4.8%-5.6%) 3 y after (2014) (p < 0.001). The average patient charge increased from US$426 in 2010 to US$551 in 2014, representing a 16% increase after adjusting for inflation in medical prices. The primary limitation to the study is that it was a pre/post-observational study with no control group that was not exposed to the law.
Ohio law required use of a medication abortion protocol that is associated with a greater need for additional intervention, more visits, more side effects, and higher costs for women relative to the evidence-based protocol. There is no evidence that the change in law led to improved abortion outcomes. Indeed, our findings suggest the opposite. In March 2016, the FDA-protocol was updated, so Ohio providers may now legally provide current evidence-based protocols. However, this law is still in place and bans physicians from using mifepristone based on any new developments in clinical research as best practices continue to be updated.
2011年2月,俄亥俄州一项法律生效,强制要求使用美国食品药品监督管理局(FDA)批准的米非司酮用药方案,该药物与米索前列醇联合用于药物流产。其他州立法机构也通过或颁布了类似法律,要求使用FDA批准的药物流产用药方案。本研究的目的是探讨这一法律变化与药物流产结局及使用情况之间的关联。
我们采用回顾性队列设计,比较法律实施前和实施后药物流产患者的结局。社会人口统计学和临床病历数据取自俄亥俄州四家提供堕胎服务的医疗机构中,从法律实施前1年(2010年1月至2011年1月)到实施后3年(2011年2月至2014年10月)的所有药物流产患者。对研究期间妊娠≤49天的所有堕胎女性的结局数据进行分析。主要结局如下:药物流产后需要额外干预的情况(如刮宫、重复使用米索前列醇和输血)、持续妊娠的频率、副作用报告以及药物流产(相对于其他堕胎程序)的比例。在2783例妊娠≤49天的药物流产中,法律实施前为4.9%(95%CI:3.7%-6.2%),法律实施后为14.3%(95%CI:12.6%-16.0%)需要一次或多次额外干预。法律实施后接受药物流产的女性需要额外干预的几率是法律实施前女性的三倍(调整后的优势比[AOR]=3.11,95%CI:2.27-4.27)。在一个以机构月为分析单位的混合效应多变量模型中,以考虑各地点缺乏独立性的情况,我们发现法律变化与需要额外干预的发生率绝对增加9.4%(95%CI:4.0%-18.4%)相关。两个时期最常见的后续干预是额外使用一剂米索前列醇,最常用于治疗不完全流产。需要两次或更多次随访的女性比例从法律实施前的4.2%(95%CI:3.0%-5.3%)增加到法律实施后的6.2%(95%CI:5.5%-8.0%)(p=0.003)。持续妊娠很少见(0.3%)。总体而言,12.6%的女性在药物流产期间报告至少一种副作用:法律实施前为8.4%(95%CI:6.8%-10.0%),法律实施后为15.6%(95%CI:13.8%-17.3%)(p<0.001)。药物流产在法律生效前一年(2010年)占所有堕胎的22%(95%CI:20.8%-22.3%),到三年后(2014年)降至5%(95%CI:4.8%-5.6%)(p<0.001)。平均患者费用从2010年时的426美元增加到2014年的551美元,表示在调整医疗价格通胀后增加了16%。本研究的主要局限性在于,它是一项无对照组的前后观察性研究,对照组未受该法律影响。
俄亥俄州法律要求使用的药物流产方案,相对于基于证据的方案,与女性需要更多额外干预、更多次就诊、更多副作用以及更高费用相关。没有证据表明法律变化导致堕胎结局改善。事实上,我们的研究结果表明情况相反。2016年3月,FDA方案进行了更新,因此俄亥俄州的医疗服务提供者现在可以合法提供当前基于证据的方案。然而,这项法律仍然有效,并且禁止医生根据临床研究的任何新进展使用米非司酮,因为最佳实践仍在不断更新。