Savastio Silvia, Cadario Francesco, Genoni Giulia, Bellomo Giorgio, Bagnati Marco, Secco Gioel, Picchi Raffaella, Giglione Enza, Bona Gianni
Division of Pediatrics, Department of Health Sciences, University of Piemonte Orientale, Novara, Italy.
IRCAD (Interdisciplinary Research Center of Autoimmune Diseases), Novara, Italy.
PLoS One. 2016 Sep 8;11(9):e0162554. doi: 10.1371/journal.pone.0162554. eCollection 2016.
Vitamin D (25OHD) effects on glycemic control are unclear in children and adolescents with type 1 diabetes. Aims of this study were to investigate 25OHD status among children with T1DM and its relationship with insulin sensitivity and glycemic status.
A cross sectional study was carried out between 2008-2014. A total of 141 patients had a T1DM >12 months diagnosis and were enrolled in the present study. Of these 35 (24.8%) were migrants and 106 (75.2%) Italians (T2). We retrospectively analyzed data at the onset of the disease (T0)(64 subjects) and 12-24 months before the last visit (T1,124 subjects). Fasting glucose, glycated hemoglobin (HbA1c), 25OHD levels and daily insulin requirement were evaluated and Cholecalciferol 1000 IU/day supplementation for the management of vitamin D insufficiency (<75 nmol/L) was systematically added.
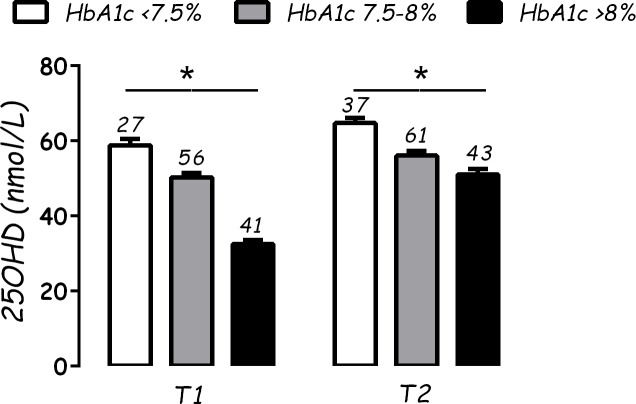
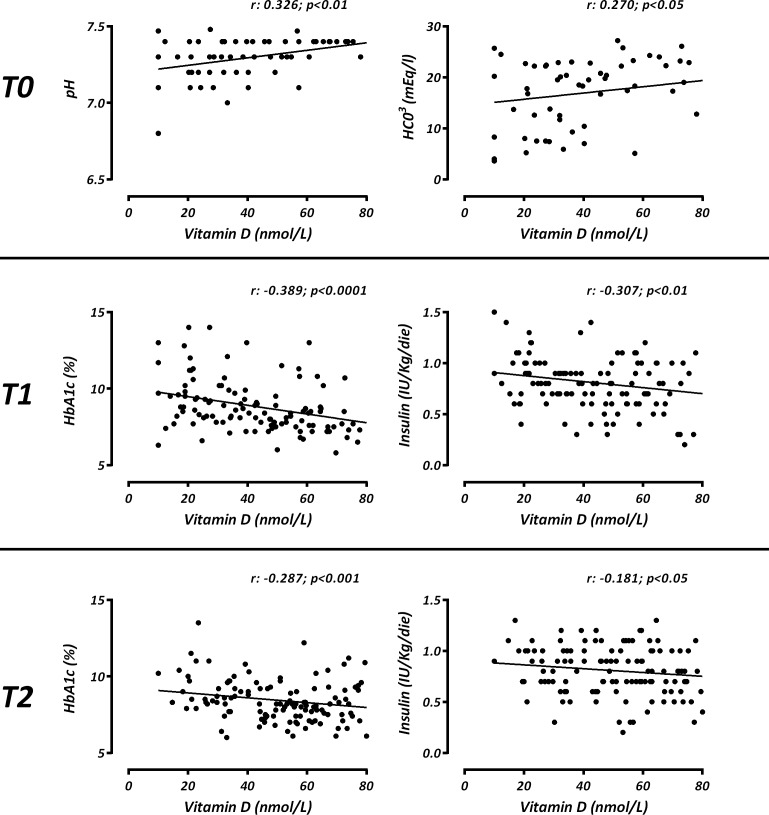
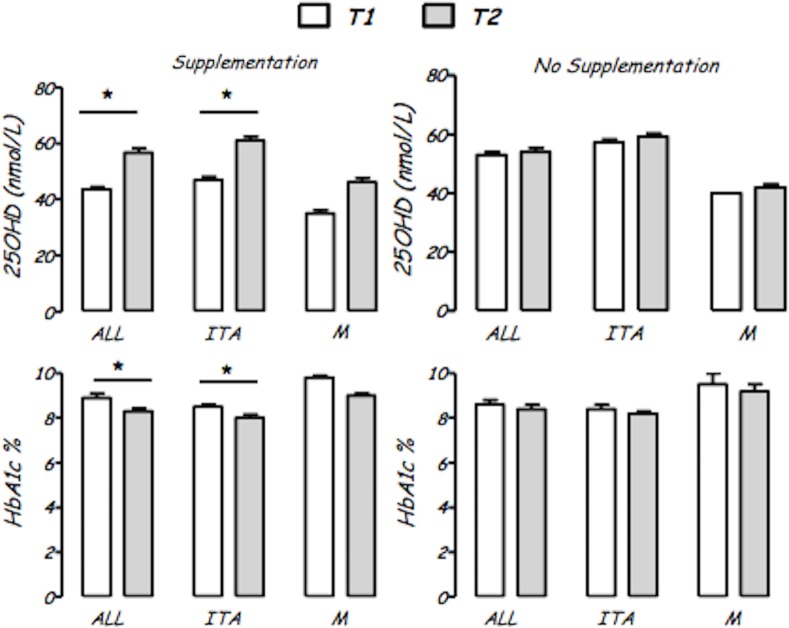
A generalized 25OHD insufficiency was found at each study time, particularly in migrants. At T0, the 25OHD levels were inversely related to diabetic keto-acidosis (DKA) severity (p<0.05). At T1 and T2, subjects with 25OHD ≤25nmol/L (10 ng/mL) showed higher daily insulin requirement (p<0.05) and HbA1c values (p<0.01) than others vitamin D status. The 25OHD levels were negatively related with HbA1c (p<0.001) and daily insulin dose (p<0.05) during follow up. There was a significant difference in 25OHD (p<0.01) between subjects with different metabolic control (HbA1c <7.5%,7.5-8%,>8%), both at T1 and T2. In supplemented subjects, we found a significant increase in 25OHD levels (p<0.0001) and decrease of HbA1c (p<0.001) between T1 and T2, but this was not significant in the migrants subgroup. Multivariate regression analysis showed a link between HbA1c and 25OHD levels (p<0.001).
Children with T1DM show a generalized 25OHD deficiency that impact on metabolic status and glycemic homeostasis. Vitamin D supplementation improves glycemic control and should be considered as an additional therapy.
1型糖尿病儿童和青少年中,维生素D(25羟维生素D)对血糖控制的影响尚不清楚。本研究旨在调查1型糖尿病患儿的25羟维生素D状态及其与胰岛素敏感性和血糖状态的关系。
于2008年至2014年进行了一项横断面研究。共有141例诊断为1型糖尿病超过12个月的患者纳入本研究。其中35例(24.8%)为移民,106例(75.2%)为意大利人(T2)。我们回顾性分析了疾病发作时(T0,64例受试者)和最后一次就诊前12 - 24个月(T1,124例受试者)的数据。评估了空腹血糖、糖化血红蛋白(HbA1c)、25羟维生素D水平和每日胰岛素需求量,并系统地添加了1000 IU/天的胆钙化醇以治疗维生素D不足(<75 nmol/L)。
在每个研究时间点均发现普遍存在25羟维生素D不足,尤其是在移民中。在T0时,25羟维生素D水平与糖尿病酮症酸中毒(DKA)严重程度呈负相关(p<0.05)。在T1和T2时,25羟维生素D≤25nmol/L(10 ng/mL)的受试者比其他维生素D状态的受试者每日胰岛素需求量更高(p<0.05),HbA1c值更高(p<0.01)。随访期间,25羟维生素D水平与HbA1c(p<0.001)和每日胰岛素剂量(p<0.05)呈负相关。在T1和T2时,不同代谢控制情况(HbA1c<7.5%、7.5 - 8%、>8%)的受试者之间25羟维生素D存在显著差异(p<0.01)。在补充维生素D的受试者中,我们发现T1和T2之间25羟维生素D水平显著升高(p<0.0001),HbA1c降低(p<0.001),但在移民亚组中不显著。多因素回归分析显示HbA1c与25羟维生素D水平之间存在关联(p<0.001)。
1型糖尿病患儿普遍存在25羟维生素D缺乏,这会影响代谢状态和血糖稳态。补充维生素D可改善血糖控制,应被视为一种辅助治疗方法。