Halimi Jean-Michel, Joly Dominique, Combe Christian, Choukroun Gabriel, Dussol Bertrand, Fauvel Jean-Pierre, Quéré Stéphane, Fiquet Béatrice
Université François-Rabelais, Faculté de Médecine, Service de Néphrologie-Immunologie Clinique, Hôpital Bretonneau, CHU Tours and EA4245, Tours, France.
Université Paris-Descartes, Faculté de Médecine, AP-HP; Service de Néphrologie, Hôpital Necker-Enfants Malades, Paris, France.
BMC Nephrol. 2016 Sep 21;17(1):135. doi: 10.1186/s12882-016-0336-1.
Type 2 diabetes (T2DM) is the leading cause of chronic kidney disease (CKD) in western countries. The combination of both increases the risk of end stage renal disease (ESRD), cardiovascular events and all-cause mortality. Early control of blood pressure (BP) and proteinuria (Pu) is crucial to slow down the progression of the CKD and prevent cardiovascular events and mortality. The primary objective of the study was to assess BP and Pu control after a 2-year follow-up in T2DM patients with CKD.
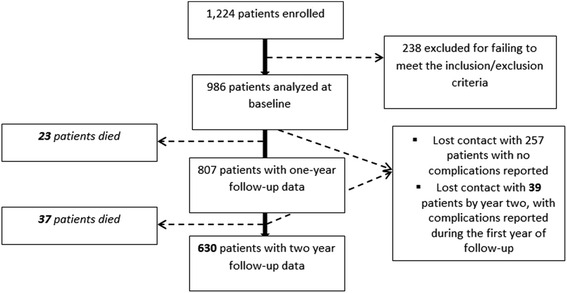
Prospective, multicenter, observational study. Overall, 153 French nephrologists included 986 T2DM patients with Pu (≥0.5 g/day) and an eGFR >15 ml/min/1.73 m. Data from 729 patients were available after a 2-year follow-up. BP and Pu control were respectively defined as less than 140/90 mmHg and 0.5 g/day. We also looked at renal and cardiovascular events.
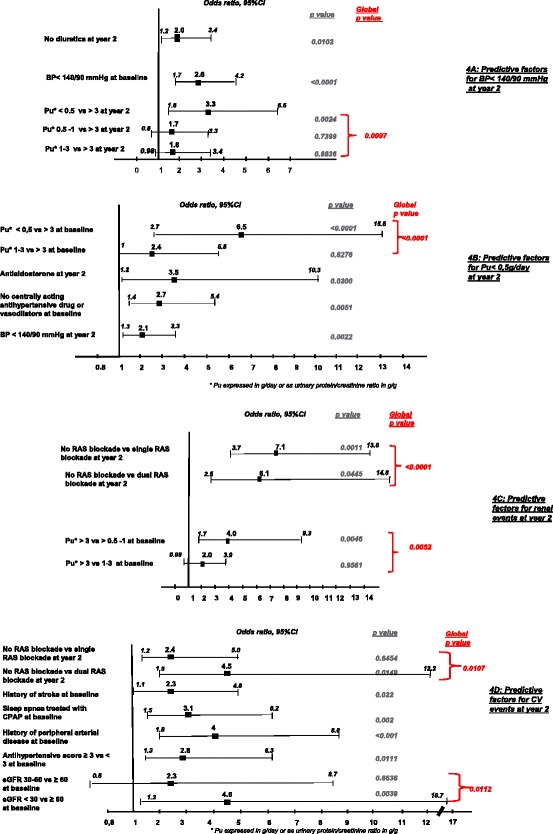
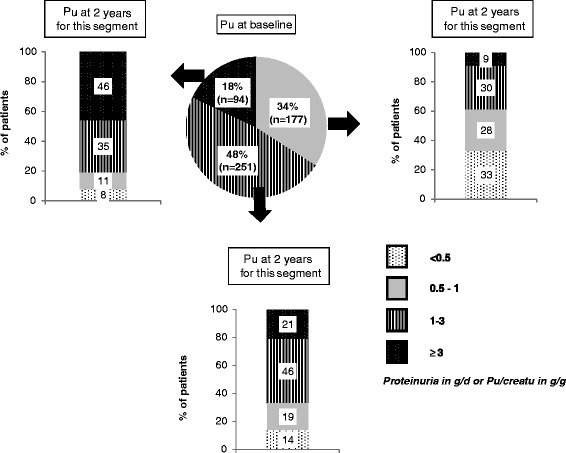
At baseline, 74 % of the patients were male, mean age was 70 years. The mean T2DM duration was 17 years with a mean HbA1c of 7.4 %. All were treated for hypertension and 33 % had a controlled BP; 81 % had dyslipidemia and LDLc was <1 g/L for 54 %; 44 % had retinopathy, 40 % macrovascular complications and 12 % heart failure. Mean Pu was 2 g/day and eGFR 40 ± 20 mL/min/1.73 m, with 13, 18, 32 and 37 % of the patients in respectively stage 2, 3a, 3b and 4 CKD. After two years, 21 % reached the Pu target and 39 % the BP target. The mean eGFR of 40 ± 20.3 ml/min/1.73 m at baseline dropped to 33.9 ± 22.6 ml/min/1.73 m by year two (p < 0.001). This corresponded to a mean annual eGFR reduction of 3.2 ml/min/1.73 m. 118 patients presented a renal event (16.2 %): doubling of serum creatinine for 86 patients (11.8 %) and start of dialysis for 72 (9.9 %); 176 patients (24.1 %) developed at least one cardiovascular complication (mainly coronary events and acute heart failure) during the follow-up period, and among these, 50 had also developed renal complications. Sixty patients died, i.e., 8.2 %, 26 patients from cardiovascular causes.
Our study highlights that achieving BP and Pu targets remains a major challenge in patients with T2DM and nephropathy. Renal failure emerges as a more frequent event than death.
2型糖尿病(T2DM)是西方国家慢性肾脏病(CKD)的主要病因。两者并存会增加终末期肾病(ESRD)、心血管事件及全因死亡率的风险。早期控制血压(BP)和蛋白尿(Pu)对于减缓CKD进展、预防心血管事件及死亡率至关重要。本研究的主要目的是评估T2DM合并CKD患者经过2年随访后的血压和蛋白尿控制情况。
前瞻性、多中心、观察性研究。共有153名法国肾脏病专家纳入了986例蛋白尿(≥0.5 g/天)且估算肾小球滤过率(eGFR)>15 ml/min/1.73 m²的T2DM患者。经过2年随访后获得了729例患者的数据。血压和蛋白尿控制分别定义为低于140/90 mmHg和0.5 g/天。我们还观察了肾脏和心血管事件。
基线时,74%的患者为男性,平均年龄70岁。T2DM平均病程为17年,平均糖化血红蛋白(HbA1c)为7.4%。所有患者均接受高血压治疗,33%的患者血压得到控制;81%的患者有血脂异常,54%的患者低密度脂蛋白胆固醇(LDLc)<1 g/L;44%的患者有视网膜病变,40%的患者有大血管并发症,12%的患者有心力衰竭。平均蛋白尿为2 g/天,eGFR为40±20 ml/min/1.73 m²,分别有13%、18%、32%和37%的患者处于CKD 2期、3a期、3b期和4期。两年后,21%的患者达到蛋白尿目标,39%的患者达到血压目标。基线时平均eGFR为40±20.3 ml/min/1.73 m²,到第二年降至33.9±22.6 ml/min/1.73 m²(p<0.001)。这相当于eGFR平均每年下降3.2 ml/min/1.73 m²。118例患者出现肾脏事件(16.2%):86例患者(11.8%)血清肌酐翻倍,72例患者(9.9%)开始透析;176例患者(24.1%)在随访期间发生至少一种心血管并发症(主要是冠状动脉事件和急性心力衰竭),其中50例患者也出现了肾脏并发症。60例患者死亡,即8.2%,26例患者死于心血管原因。
我们的研究强调,在T2DM和肾病患者中实现血压和蛋白尿目标仍然是一项重大挑战。肾衰竭比死亡更为常见。