Posma Rene A, Lexis Chris P H, Lipsic Erik, Nijsten Maarten W N, Damman Kevin, Touw Daan J, van Veldhuisen Dirk Jan, van der Harst Pim, van der Horst Iwan C C
Cardiovasc Drugs Ther. 2015;29(5):451-9. doi: 10.1007/s10557-015-6618-1.
The association between metformin use and renal function needs further to be elucidated since data are insufficient whether metformin affects renal function in higher risk populations such as after ST-elevation myocardial infarction (STEMI).
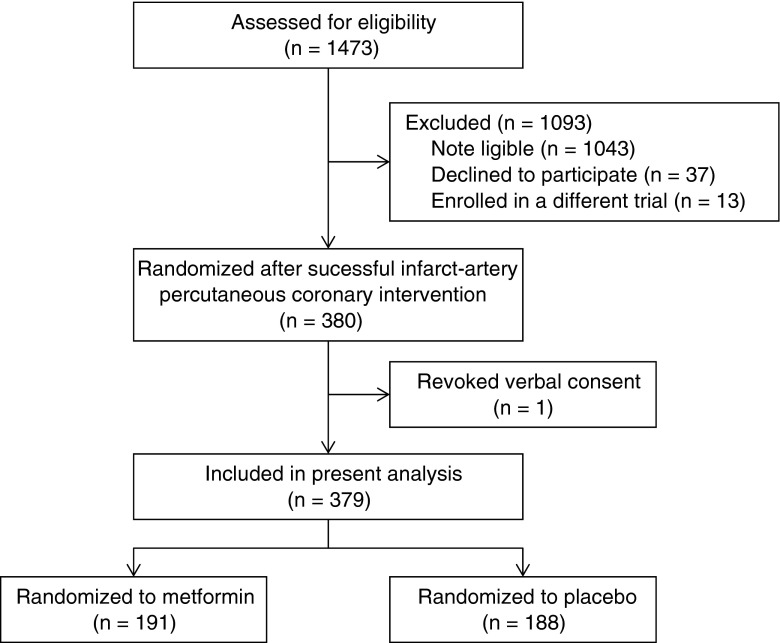
We studied 379 patients included in the GIPS-III trial in which patients without diabetes or renal dysfunction, who underwent primary percutaneous coronary interventions (PCI) for STEMI, were randomized to metformin 500 mg or placebo twice daily for four months. At baseline and at seven scheduled visits up to four months after PCI, estimated glomerular filtration rate (eGFR) was determined (2582 values). Contrast-induced acute kidney injury (CI-AKI) was defined as an increase in serum creatinine of ≥0.3 mg/dl or 25 % rise within 48 h after PCI.
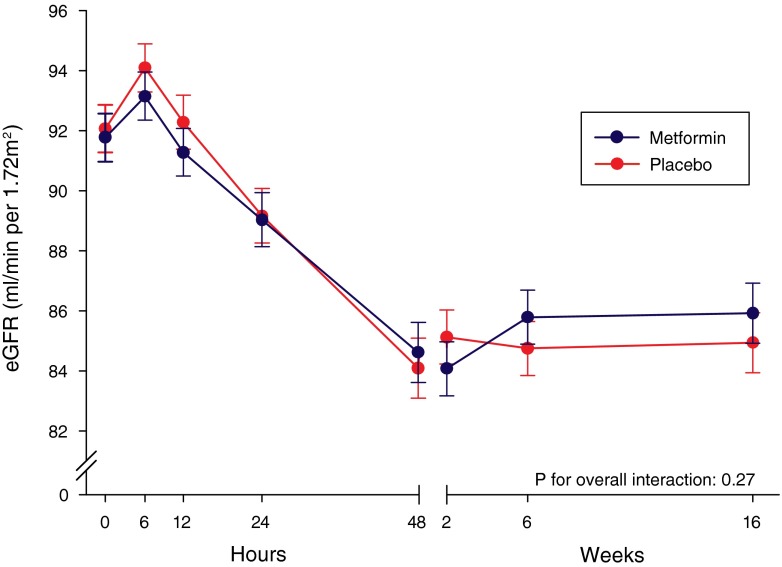
At all visits, the mean eGFR was similar in patients randomized to metformin or placebo. Over the four month period, mixed-effect repeated-measures model analysis showed a least-squares mean ± standard error change in eGFR of -5.9±0.8 ml/min/1.73 m2 in the metformin group and −7.1 ±0.8 ml/min/1.73 m2 in the control group (P=0.27 for overall interaction). The incidence of CI-AKI was 14.8 %; 29 (15.2 %) patients in the metformin group versus 27 (14.4 %) controls (P=0.89). After adjustment for covariates, metformin treatment was not associated with CI-AKI (odds ratio: 0.96, 95%CI 0.52−1.75, P=0.88).
We conclude that initiation of metformin shortly after primary PCI has no adverse effect on renal function in patients without diabetes or prior renal impairment, further providing evidence of the safety of metformin use after myocardial infarction and subsequent contrast exposure.
由于在ST段抬高型心肌梗死(STEMI)等高危人群中,关于二甲双胍是否影响肾功能的数据不足,因此二甲双胍使用与肾功能之间的关联尚需进一步阐明。
我们研究了纳入GIPS-III试验的379例患者,这些患者无糖尿病或肾功能不全,因STEMI接受了直接经皮冠状动脉介入治疗(PCI),被随机分为每日两次服用500 mg二甲双胍或安慰剂,共四个月。在基线以及PCI后四个月内的七次预定访视时,测定估计肾小球滤过率(eGFR)(共2582个值)。造影剂诱发的急性肾损伤(CI-AKI)定义为PCI后48小时内血清肌酐升高≥0.3 mg/dl或升高25%。
在所有访视中,随机分配至二甲双胍组或安慰剂组的患者的平均eGFR相似。在四个月期间,混合效应重复测量模型分析显示,二甲双胍组eGFR的最小二乘均值±标准误变化为-5.9±0.8 ml/min/1.73 m²,对照组为-7.1±0.8 ml/min/1.73 m²(总体交互作用P = 0.27)。CI-AKI的发生率为14.8%;二甲双胍组有29例(15.2%)患者,对照组有27例(14.4%)患者(P = 0.89)。在对协变量进行调整后,二甲双胍治疗与CI-AKI无关(比值比:0.96,95%CI 0.52 - 1.75,P = 0.88)。
我们得出结论,在直接PCI后不久开始使用二甲双胍,对无糖尿病或既往无肾功能损害的患者的肾功能没有不利影响,进一步提供了心肌梗死后使用二甲双胍以及随后接受造影剂的安全性证据。