Njom Nlend Anne Esther, Nguwoh Philippe Salomon, Ngounouh Christian Taheu, Tchidjou Hyppolite Kuekou, Pieme Constant Anatole, Otélé Jean Mbede, Penlap Véronique, Colizzi Vittorio, Moyou Roger Somo, Fokam Joseph
Pediatric Service, National Insurance Fund Welfare Hospital, Yaoundé, Cameroon.
Faculty of Medicine and Biomedical Sciences, University of Yaoundé 1, Yaoundé, Cameroon.
PLoS One. 2016 Sep 22;11(9):e0161714. doi: 10.1371/journal.pone.0161714. eCollection 2016.
Since 2005, anti-hepatitis B virus (anti-HBV) vaccine is part of the Expanded Program on Immunization (EPI) for infants born in Cameroon, with 99% anti-HBV coverage. In a context of generalized HIV epidemiology, we assessed paediatric anti-HBV vaccine response according to HIV status, feeding option and age in a tropical context.
Prospective, observational and cross-sectional study conducted among 82 children (27 [IQR: 9-47] months, min-max: 6-59), after complete anti-HBV vaccination (Zilbrix Hepta: 10μg AgHBs) at the Essos Health Centre in Yaounde, Cameroon, classified as group-A: HIV unexposed (28), group-B: HIV-exposed/uninfected (29), group-C: HIV-infected (25). Quantitative anti-HBs ELISA was interpreted as "no", "low-" or "protective-response" with <1, 1-10, or ≥10 IU/L respectively; with p-value<0.05 considered significant.
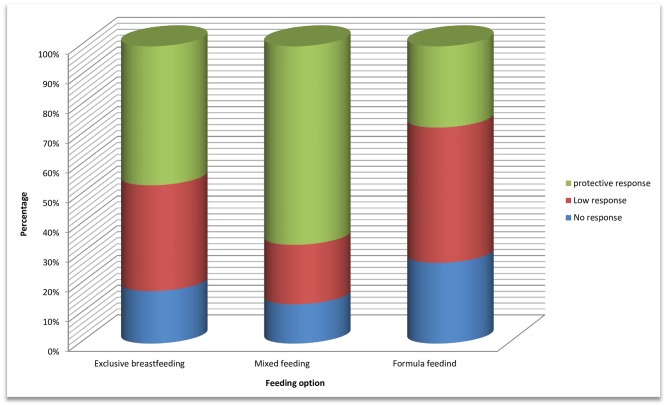
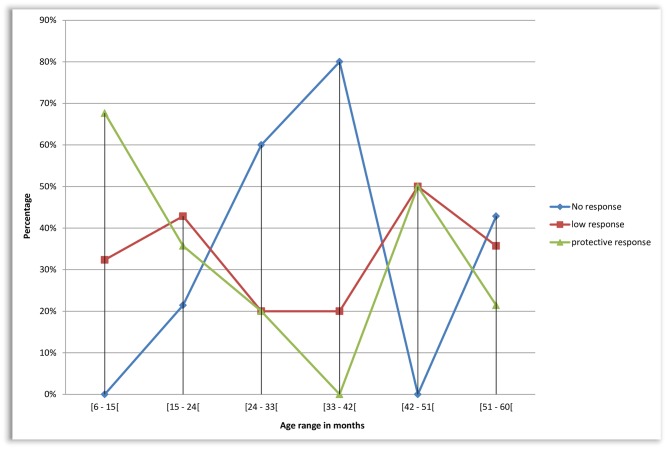
Children were all HBV-unexposed (AcHBc-negative) and uninfected (HBsAg-negative). Response to anti-HBV vaccine was 80.49% (66/82), with only 45.12% (37/82) developed a protective-response (≥10IU/L). According to HIV status, 60.71% (17/28) developed a protective-response in group-A, vs. 51.72% (15/29) and 20% (5/25) in group-B and group-C respectively, Odds Ratio (OR): 2.627 [CI95% 0.933-7.500], p = 0.041. According to feeding option during first six months of life, 47.67% (21/45) developed a protective-response on exclusive breastfeeding vs. 43.24% (16/37) on mixed or formula feeding, OR: 1.148 [CI95% 0.437-3.026], p = 0.757. According to age, protective-response decreased significantly as children grow older: 58.33% (28/48) <24 months vs. 26.47% (9/34) ≥24 months, OR: 3.889 [CI95% 1.362-11.356], p = 0.004; and specifically 67.65% (23/34) ≤6 months vs. 0%, (0/5) 33-41 months, p = 0.008.
Anti-HBV vaccine provides low rate of protection (<50%) among children in general, and particularly if HIV-exposed, infected and/or older children. Implementing policies for early vaccination, specific immunization algorithm for HIV-exposed/infected children, and monitoring vaccine response would ensure effective protection in tropical settings, pending extensive/confirmatory investigations.
自2005年以来,抗乙肝病毒(anti-HBV)疫苗成为喀麦隆出生婴儿扩大免疫规划(EPI)的一部分,抗HBV疫苗接种率达99%。在艾滋病病毒广泛流行的背景下,我们在热带地区根据儿童的艾滋病毒感染状况、喂养方式和年龄评估了小儿抗HBV疫苗的反应。
在喀麦隆雅温得的埃索斯健康中心对82名儿童(年龄中位数[四分位间距:9 - 47]个月,最小 - 最大年龄:6 - 59个月)进行了前瞻性、观察性和横断面研究,这些儿童在完成抗HBV疫苗接种(Zilbrix Hepta:10μg重组乙肝表面抗原)后,被分为A组:未接触艾滋病毒(28名),B组:接触艾滋病毒/未感染(29名),C组:感染艾滋病毒(25名)。定量抗HBs ELISA检测结果分别以<1、1 - 10或≥10 IU/L解释为“无”、“低”或“保护性反应”;p值<0.05被认为具有统计学意义。
所有儿童均未接触过乙肝病毒(抗HBc阴性)且未感染(HBsAg阴性)。抗HBV疫苗的反应率为80.49%(66/82),只有45.12%(37/82)产生了保护性反应(≥10 IU/L)。根据艾滋病毒感染状况,A组60.71%(17/28)产生了保护性反应,而B组和C组分别为51.72%(15/29)和20%(5/25),优势比(OR):2.627 [95%置信区间0.933 - 7.500],p = 0.041。根据出生后头六个月的喂养方式,纯母乳喂养的儿童中有47.67%(21/45)产生了保护性反应,混合或配方奶喂养的儿童中这一比例为43.24%(16/37),OR:1.148 [95%置信区间0.437 - 3.026],p = 0.757。根据年龄,随着儿童年龄增长,保护性反应显著降低:<24个月的儿童中有58.33%(28/48)产生了保护性反应,≥24个月的儿童中这一比例为26.47%(9/34),OR:3.889 [95%置信区间1.362 - 11.356],p = 0.004;具体而言,≤6个月的儿童中有67.65%(23/34)产生了保护性反应,33 - 41个月的儿童中这一比例为0%(0/5),p = 0.008。
总体而言,抗HBV疫苗在儿童中的保护率较低(<50%),尤其是对于接触艾滋病毒、感染艾滋病毒的儿童和/或年龄较大的儿童。在进行广泛/验证性调查之前,实施早期疫苗接种政策、针对接触艾滋病毒/感染艾滋病毒儿童的特定免疫算法以及监测疫苗反应将确保在热带地区提供有效的保护。