Mares Marie-Louise, Gustafson David H, Glass Joseph E, Quanbeck Andrew, McDowell Helene, McTavish Fiona, Atwood Amy K, Marsch Lisa A, Thomas Chantelle, Shah Dhavan, Brown Randall, Isham Andrew, Nealon Mary Jane, Ward Victoria
Department of Communication Arts, University of Wisconsin-Madison, Madison, WI, 53706, USA.
Center for Health Enhancement System Studies, University of Wisconsin-Madison, Madison, WI, 53706, USA.
BMC Med Inform Decis Mak. 2016 Sep 29;16(1):126. doi: 10.1186/s12911-016-0365-5.
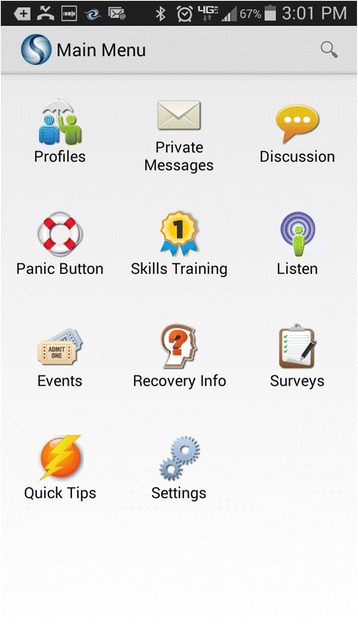
Millions of Americans need but don't receive treatment for substance use, and evidence suggests that addiction-focused interventions on smart phones could support their recovery. There is little research on implementation of addiction-related interventions in primary care, particularly in Federally Qualified Health Centers (FQHCs) that provide primary care to underserved populations. We used mixed methods to examine three FQHCs' implementation of Seva, a smart-phone app that offers patients online support/discussion, health-tracking, and tools for coping with cravings, and offers clinicians information about patients' health tracking and relapses. We examined (a) clinicians' initial perspectives about implementing Seva, and (b) the first year of implementation at Site 1.
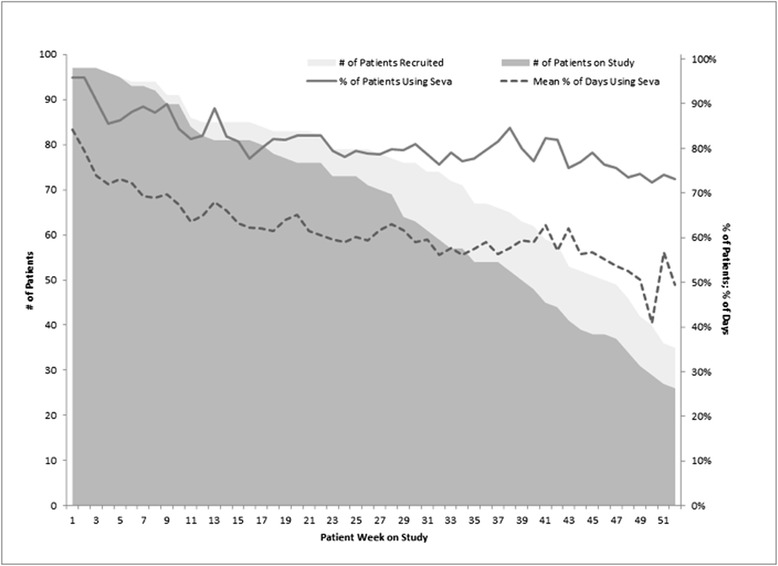
Prior to staggered implementation at three FQHCs (Midwest city in WI vs. rural town in MT vs. metropolitan NY), interviews, meetings, and focus groups were conducted with 53 clinicians to identify core themes of initial expectations about implementation. One year into implementation at Site 1, clinicians there were re-interviewed. Their reports were supplemented by quantitative data on clinician and patient use of Seva.
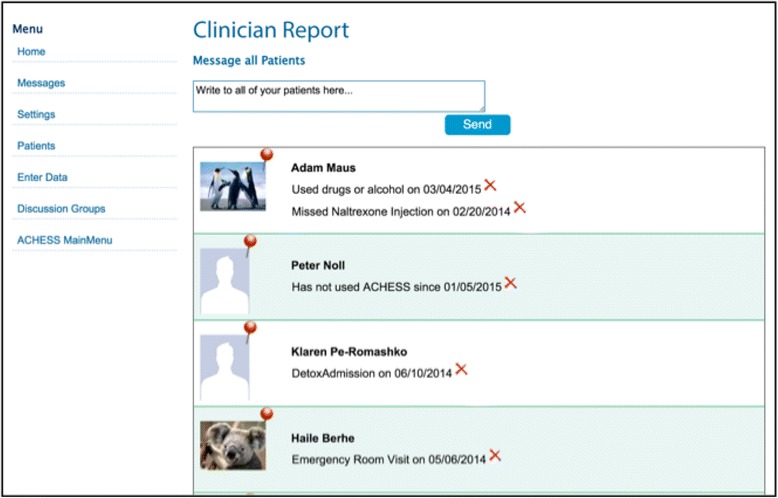
Clinicians anticipated that Seva could help patients and make behavioral health appointments more efficient, but they were skeptical that physicians would engage with Seva (given high caseloads), and they were uncertain whether patients would use Seva. They were concerned about legal obligations for monitoring patients' interactions online, including possible "cries for help" or inappropriate interactions. One year later at Site 1, behavioral health care providers, rather than physicians, had incorporated Seva into patient care, primarily by discussing it during appointments. Given workflow/load concerns, only a few key clinicians monitored health tracking/relapses and prompted outreach when needed; two researchers monitored the discussion board and alerted the clinic as needed. Clinician turnover/leave complicated this approach. Contrary to clinicians' initial concerns, patients showed sustained, mutually supportive use of Seva, with few instances of misuse.
Results suggest the value of (a) focusing implementation on behavioral health care providers rather than physicians, (b) assigning a few individuals (not necessarily clinicians) to monitor health tracking, relapses, and the discussion board, (c) anticipating turnover/leave and having designated replacements. Patients showed sustained, positive use of Seva.
ClinicalTrials.gov ( NCT01963234 ).
数以百万计的美国人需要但未接受物质使用治疗,且有证据表明,针对成瘾问题的智能手机干预措施有助于他们康复。关于在初级保健中实施与成瘾相关干预措施的研究很少,尤其是在为服务不足人群提供初级保健的联邦合格健康中心(FQHCs)。我们采用混合方法研究了三家FQHCs对Seva的实施情况,Seva是一款智能手机应用程序,为患者提供在线支持/讨论、健康追踪以及应对渴望的工具,并为临床医生提供有关患者健康追踪和复发的信息。我们研究了(a)临床医生对实施Seva的初步看法,以及(b)在1号地点实施的第一年情况。
在三家FQHCs(威斯康星州的中西部城市、蒙大拿州的乡村小镇和纽约市)交错实施之前,对53名临床医生进行了访谈、会议和焦点小组讨论,以确定对实施的初步期望的核心主题。在1号地点实施一年后,对那里的临床医生进行了再次访谈。他们的报告得到了关于临床医生和患者使用Seva的定量数据的补充。
临床医生预计Seva可以帮助患者并提高行为健康预约的效率,但他们怀疑医生是否会使用Seva(鉴于工作量大),并且不确定患者是否会使用Seva。他们担心在线监测患者互动的法律义务,包括可能的“求助呼声”或不当互动。一年后在1号地点,行为健康护理提供者而非医生将Seva纳入患者护理,主要是在预约期间进行讨论。鉴于工作流程/工作量问题,只有少数关键临床医生监测健康追踪/复发情况,并在需要时促使进行外展;两名研究人员监测讨论板并在需要时向诊所发出警报。临床医生的更替/离职使这种方法变得复杂。与临床医生最初的担忧相反,患者持续、相互支持地使用Seva,很少有滥用情况。
结果表明(a)将实施重点放在行为健康护理提供者而非医生身上,(b)指定少数人(不一定是临床医生)监测健康追踪、复发情况和讨论板,(c)预期更替/离职并指定替代人员的价值。患者持续、积极地使用Seva。
ClinicalTrials.gov(NCT01963234)。