Desautels Thomas, Calvert Jacob, Hoffman Jana, Jay Melissa, Kerem Yaniv, Shieh Lisa, Shimabukuro David, Chettipally Uli, Feldman Mitchell D, Barton Chris, Wales David J, Das Ritankar
Dascena, Inc, Hayward, CA, United States.
Department of Clinical Informatics, Stanford University School of Medicine, Stanford, CA, United States
JMIR Med Inform. 2016 Sep 30;4(3):e28. doi: 10.2196/medinform.5909.
Sepsis is one of the leading causes of mortality in hospitalized patients. Despite this fact, a reliable means of predicting sepsis onset remains elusive. Early and accurate sepsis onset predictions could allow more aggressive and targeted therapy while maintaining antimicrobial stewardship. Existing detection methods suffer from low performance and often require time-consuming laboratory test results.
To study and validate a sepsis prediction method, InSight, for the new Sepsis-3 definitions in retrospective data, make predictions using a minimal set of variables from within the electronic health record data, compare the performance of this approach with existing scoring systems, and investigate the effects of data sparsity on InSight performance.
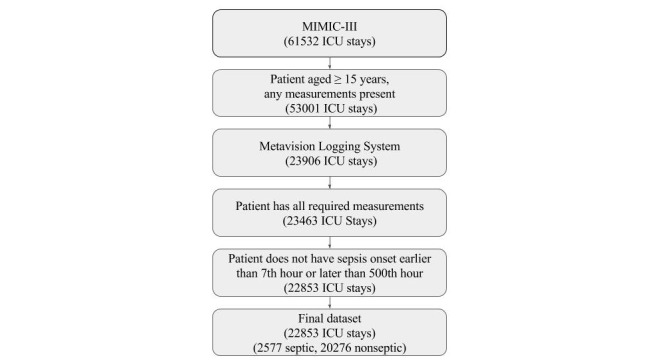
We apply InSight, a machine learning classification system that uses multivariable combinations of easily obtained patient data (vitals, peripheral capillary oxygen saturation, Glasgow Coma Score, and age), to predict sepsis using the retrospective Multiparameter Intelligent Monitoring in Intensive Care (MIMIC)-III dataset, restricted to intensive care unit (ICU) patients aged 15 years or more. Following the Sepsis-3 definitions of the sepsis syndrome, we compare the classification performance of InSight versus quick sequential organ failure assessment (qSOFA), modified early warning score (MEWS), systemic inflammatory response syndrome (SIRS), simplified acute physiology score (SAPS) II, and sequential organ failure assessment (SOFA) to determine whether or not patients will become septic at a fixed period of time before onset. We also test the robustness of the InSight system to random deletion of individual input observations.
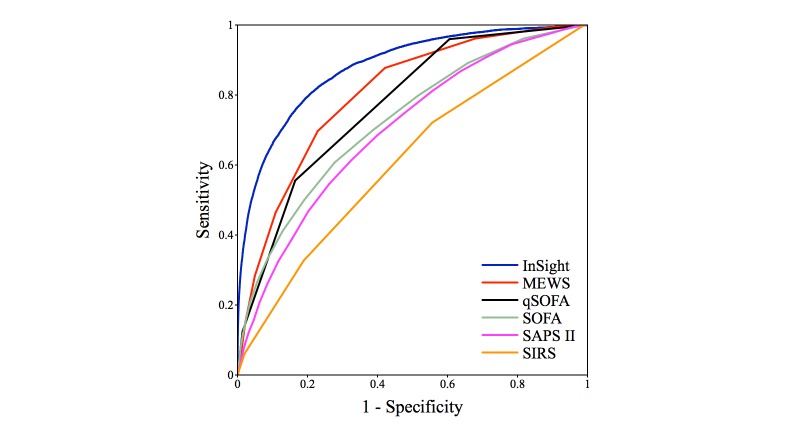
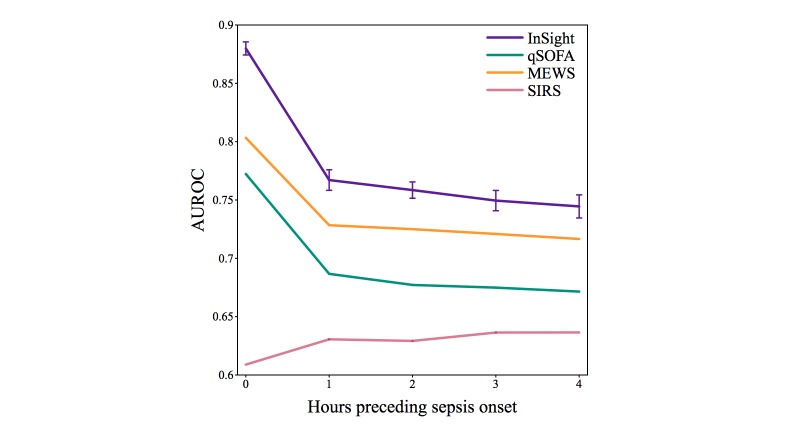
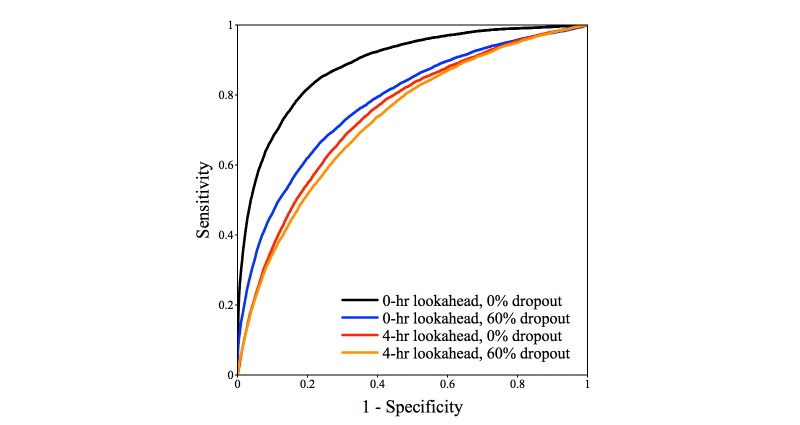
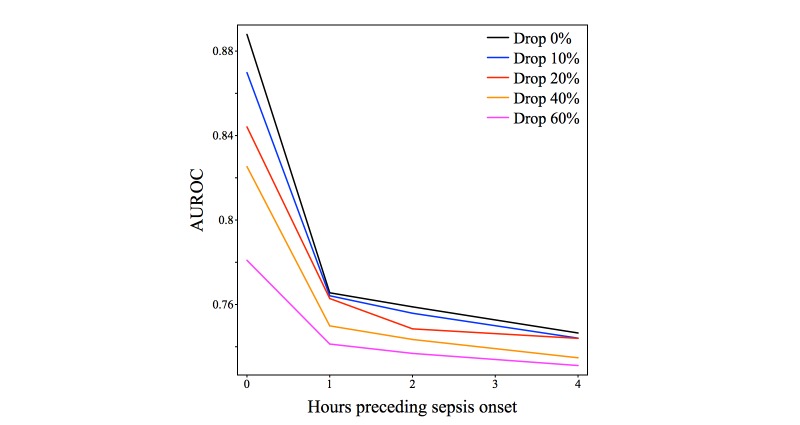
In a test dataset with 11.3% sepsis prevalence, InSight produced superior classification performance compared with the alternative scores as measured by area under the receiver operating characteristic curves (AUROC) and area under precision-recall curves (APR). In detection of sepsis onset, InSight attains AUROC = 0.880 (SD 0.006) at onset time and APR = 0.595 (SD 0.016), both of which are superior to the performance attained by SIRS (AUROC: 0.609; APR: 0.160), qSOFA (AUROC: 0.772; APR: 0.277), and MEWS (AUROC: 0.803; APR: 0.327) computed concurrently, as well as SAPS II (AUROC: 0.700; APR: 0.225) and SOFA (AUROC: 0.725; APR: 0.284) computed at admission (P<.001 for all comparisons). Similar results are observed for 1-4 hours preceding sepsis onset. In experiments where approximately 60% of input data are deleted at random, InSight attains an AUROC of 0.781 (SD 0.013) and APR of 0.401 (SD 0.015) at sepsis onset time. Even with 60% of data missing, InSight remains superior to the corresponding SIRS scores (AUROC and APR, P<.001), qSOFA scores (P=.0095; P<.001) and superior to SOFA and SAPS II computed at admission (AUROC and APR, P<.001), where all of these comparison scores (except InSight) are computed without data deletion.
Despite using little more than vitals, InSight is an effective tool for predicting sepsis onset and performs well even with randomly missing data.
脓毒症是住院患者死亡的主要原因之一。尽管如此,预测脓毒症发作的可靠方法仍然难以捉摸。早期准确的脓毒症发作预测可以在维持抗菌药物管理的同时,实现更积极、更有针对性的治疗。现有的检测方法性能较低,且往往需要耗时的实验室检测结果。
研究并验证一种针对脓毒症新定义(Sepsis-3)的脓毒症预测方法InSight,使用电子健康记录数据中的最少变量集进行预测,将该方法的性能与现有评分系统进行比较,并研究数据稀疏性对InSight性能的影响。
我们应用InSight,这是一种机器学习分类系统,使用易于获取的患者数据(生命体征、外周毛细血管血氧饱和度、格拉斯哥昏迷评分和年龄)的多变量组合,通过回顾性重症监护多参数智能监测(MIMIC)-III数据集来预测脓毒症,该数据集仅限于15岁及以上的重症监护病房(ICU)患者。按照脓毒症综合征的Sepsis-3定义,我们比较了InSight与快速序贯器官衰竭评估(qSOFA)、改良早期预警评分(MEWS)、全身炎症反应综合征(SIRS)、简化急性生理学评分(SAPS)II和序贯器官衰竭评估(SOFA)的分类性能,以确定患者在发作前的固定时间段内是否会发生脓毒症。我们还测试了InSight系统对随机删除单个输入观测值的稳健性。
在脓毒症患病率为11.3%的测试数据集中,与通过受试者工作特征曲线下面积(AUROC)和精确召回率曲线下面积(APR)衡量的其他评分相比,InSight产生了卓越的分类性能。在检测脓毒症发作时,InSight在发作时的AUROC = 0.880(标准差0.006),APR = 0.595(标准差0.016),两者均优于同期计算的SIRS(AUROC:0.609;APR:0.160)、qSOFA(AUROC:0.772;APR:0.277)和MEWS(AUROC:0.803;APR:0.327),以及入院时计算的SAPS II(AUROC:0.700;APR:0.225)和SOFA(AUROC:0.725;APR:0.284)(所有比较P<0.001)。在脓毒症发作前1-4小时也观察到了类似结果。在随机删除约60%输入数据的实验中,InSight在脓毒症发作时的AUROC为0.781(标准差0.013),APR为0.401(标准差0.015)。即使有60%的数据缺失,InSight仍然优于相应的SIRS评分(AUROC和APR,P<0.001)、qSOFA评分(P = 0.0095;P<0.001),并且优于入院时计算的SOFA和SAPS II(AUROC和APR,P<0.001),其中所有这些比较评分(InSight除外)都是在不删除数据的情况下计算的。
尽管InSight使用的数据仅略多于生命体征,但它是预测脓毒症发作的有效工具,即使在数据随机缺失的情况下也表现良好。