Department of Internal Medicine, Division of Gastroenterology and Hepatology, Medical University of Graz, Graz, Austria.
Department of Internal Medicine, Clinical Division of Nephrology, Medical University of Graz, Graz, Austria.
Sci Rep. 2016 Oct 4;6:34534. doi: 10.1038/srep34534.
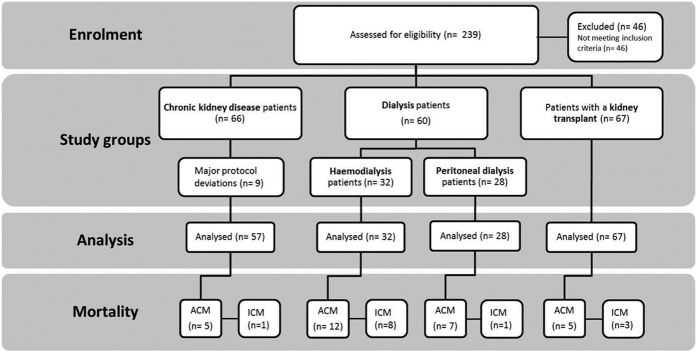
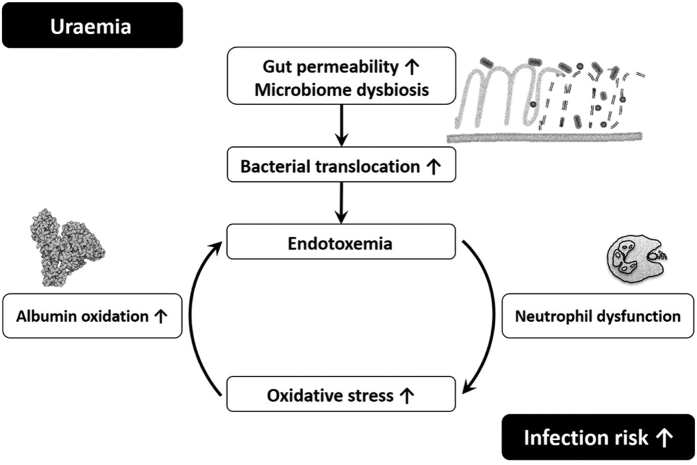
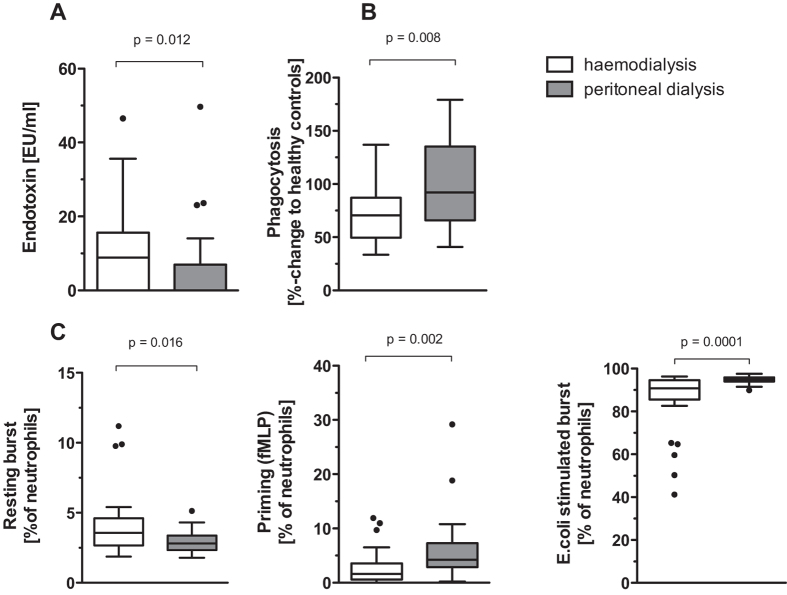
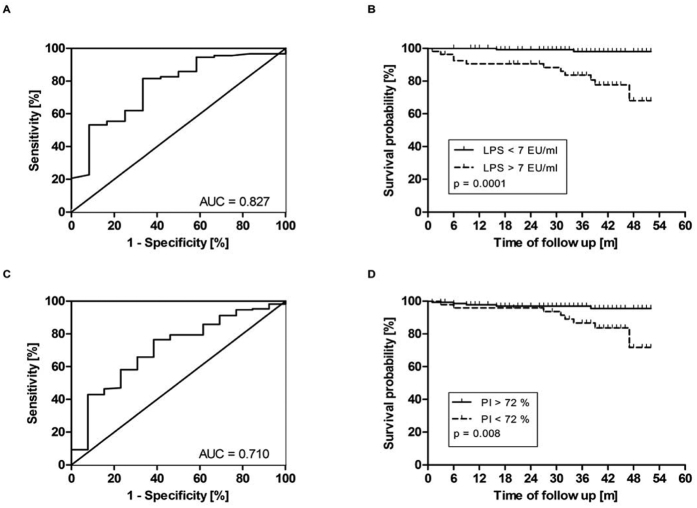
Bacterial infection and sepsis are common complications of chronic kidney disease (CKD). A vicious cycle of increased gut permeability, endotoxemia, inadequate activation of the innate immune system and resulting innate immune dysfunction is hypothesized. We assessed endotoxemia, neutrophil function and its relation to oxidative stress, inflammation and gut permeability in patients with CKD grade 3-5 without renal replacement therapy (CKD group, n = 57), patients with CKD stage 5 undergoing haemodialysis (HD, n = 32) or peritoneal dialysis (PD, n = 28) and patients after kidney transplantation (KT, n = 67) in a cross-sectional observational study. In HD patients, endotoxin serum levels were elevated and neutrophil phagocytic capacity was decreased compared to all other groups. Patients on HD had a significantly higher mortality, due to infections during follow up, compared to PD (p = 0.022). Oxidative stress, neutrophil energy charge, systemic inflammation and gut permeability could not completely explain these differences. Our findings suggest that dialysis modality and not renal function per se determine the development of neutrophil dysfunction and endotoxemia in CKD-patients. HD patients are particularly prone to neutrophil dysfunction and endotoxemia whereas neutrophil function seems to improve after KT. Multi-target approaches are therefore warranted to improve neutrophil function and potentially reduce the rate of infections with patients undergoing haemodialysis.
细菌感染和败血症是慢性肾脏病(CKD)的常见并发症。人们假设,肠道通透性增加、内毒素血症、固有免疫系统激活不足以及由此导致的固有免疫功能障碍之间存在恶性循环。我们在一项横断面观察性研究中评估了 3-5 期未接受肾脏替代治疗的 CKD 患者(CKD 组,n=57)、接受血液透析(HD)的 CKD 5 期患者(n=32)或腹膜透析(PD)的患者(n=28)和肾移植后患者(KT,n=67)的内毒素血症、中性粒细胞功能及其与氧化应激、炎症和肠道通透性的关系。与其他所有组相比,HD 患者的血清内毒素水平升高,中性粒细胞吞噬能力下降。与 PD 相比(p=0.022),HD 患者在随访期间因感染导致的死亡率显著更高。氧化应激、中性粒细胞能量状态、全身炎症和肠道通透性不能完全解释这些差异。我们的研究结果表明,透析方式而不是肾功能本身决定了 CKD 患者中性粒细胞功能障碍和内毒素血症的发展。HD 患者尤其容易发生中性粒细胞功能障碍和内毒素血症,而中性粒细胞功能似乎在 KT 后得到改善。因此,需要采用多靶点方法来改善中性粒细胞功能,并可能降低接受血液透析患者的感染率。