Huang Wen-Juan, Chen Wei-Wei, Zhang Xia
Department of Neurology, Xuzhou Central Hospital, Xuzhou, Jiangsu 221009, P.R. China.
Oncol Lett. 2016 Oct;12(4):2283-2288. doi: 10.3892/ol.2016.4952. Epub 2016 Aug 4.
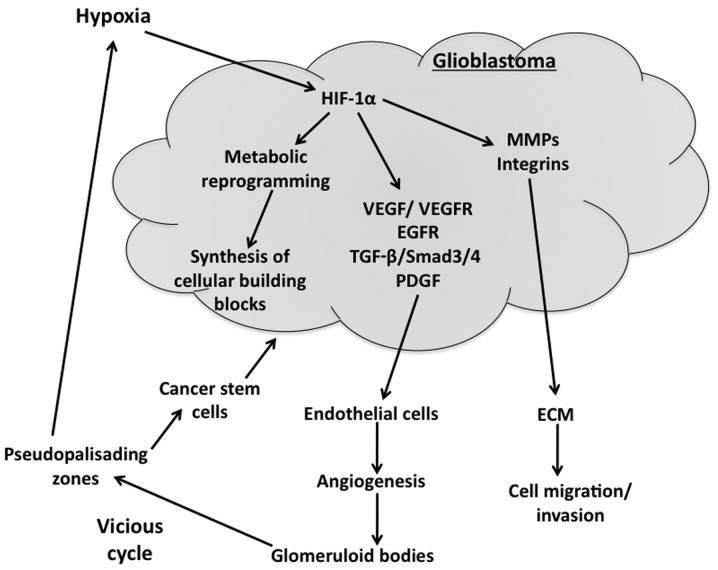
Central nervous system-based cancers have a much higher mortality rate with the 2016 estimates at 6.4 for incidence and 4.3 for deaths per 100,000 individuals. Grade IV astrocytomas, known as glioblastomas are highly aggressive and show a high proliferation index, diffused infiltration, angiogenesis, microvascular proliferation and pleomorphic vessels, resistance to apoptosis, and pseudopalisading necrosis. Extensive hypoxic regions in glioblastomas contribute to the highly malignant phenotype of these tumors. Hypoxic regions of glioblastoma exacerbate the prognosis and clinical outcomes of the patients as hypoxic tumor cells are resistant to chemo- and radiation therapy and are also protected by the malfunctional vasculature that developed due to hypoxia. Predominantly, hypoxia-inducible factor-1α, vascular endothelial growth factor (VEGF)/VEGF receptor, transforming growth factor-β, epidermal growth factor receptor and PI3 kinase/Akt signaling systems are involved in tumor progression and growth. Glioblastomas are predominantly glycolytic and hypoxia-induced factors are useful in the metabolic reprogramming of these tumors. Abnormal vessel formation is crucial in generating pseudopalisading necrosis regions that protect cancer stem cells residing in that region from therapeutic agents and this facilitates the cancer stem cell niche to expand and contribute to cell proliferation and tumor growth. Therapeutic approaches that target hypoxia-induced factors, such as use of the monoclonal antibody against VEGF, bevacizumab, have been useful only in stabilizing the disease but failed to increase overall survival. Hypoxia-activated TH-302, a nitroimidazole prodrug of cytotoxin bromo-isophosphoramide mustard, appears to be more attractive due to its better beneficial effects in glioblastoma patients. A better understanding of the hypoxia-mediated protection of glioblastoma cells is required for developing more effective therapeutics.
基于中枢神经系统的癌症死亡率要高得多,2016年的估计发病率为每10万人6.4例,死亡率为每10万人4.3例。IV级星形细胞瘤,即胶质母细胞瘤,具有高度侵袭性,增殖指数高,呈弥漫性浸润、血管生成、微血管增殖和血管多形性,抗凋亡,以及假栅栏状坏死。胶质母细胞瘤中广泛的缺氧区域导致了这些肿瘤的高度恶性表型。胶质母细胞瘤的缺氧区域会使患者的预后和临床结果恶化,因为缺氧的肿瘤细胞对化疗和放疗具有抗性,并且还受到因缺氧而发育不良的脉管系统的保护。主要地,缺氧诱导因子-1α、血管内皮生长因子(VEGF)/VEGF受体、转化生长因子-β、表皮生长因子受体和PI3激酶/Akt信号系统参与肿瘤进展和生长。胶质母细胞瘤主要进行糖酵解,缺氧诱导因子在这些肿瘤的代谢重编程中起作用。异常血管形成对于产生假栅栏状坏死区域至关重要,该区域可保护驻留在该区域的癌症干细胞免受治疗剂的影响,这有助于癌症干细胞生态位扩展并促进细胞增殖和肿瘤生长。针对缺氧诱导因子的治疗方法,如使用抗VEGF单克隆抗体贝伐单抗,仅在稳定病情方面有用,但未能提高总生存率。缺氧激活的TH-302,一种细胞毒素溴异磷酰胺芥末的硝基咪唑前药,由于其在胶质母细胞瘤患者中具有更好的有益效果,似乎更具吸引力。为了开发更有效的治疗方法,需要更好地理解缺氧介导的胶质母细胞瘤细胞保护机制。