Kyari Fatima, Nolan Winifred, Gilbert Clare
Department of Clinical Research, London School of Hygiene and Tropical Medicine, International Centre for Eye Health, London, UK Department of Ophthalmology, College of Health Sciences, University of Abuja, Abuja, Nigeria.
Moorfields Eye Hospital, London, UK.
BMJ Open. 2016 Oct 11;6(10):e012230. doi: 10.1136/bmjopen-2016-012230.
Glaucoma, a chronic non-communicable disease, and leading cause of irreversible blindness worldwide is a public health problem in Nigeria, with a prevalence of 5.02% in people aged ≥40 years. The purpose of this nationwide survey was to assess Nigerian ophthalmologists' practice patterns and their constraints in managing glaucoma.
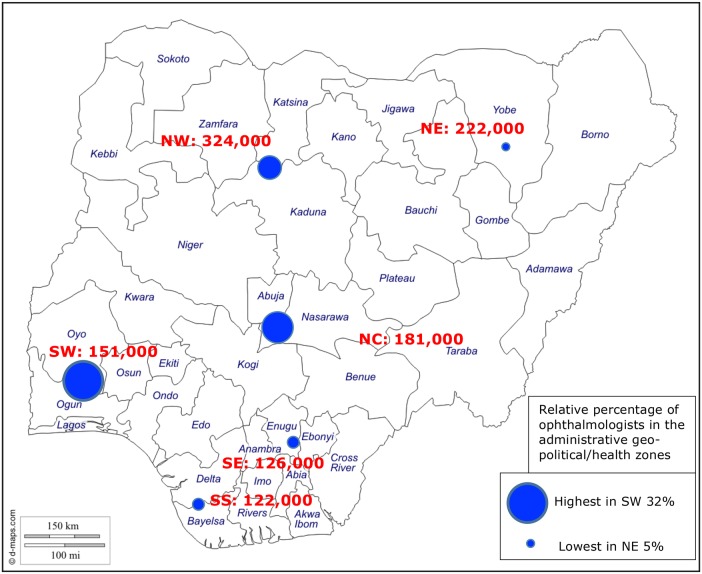
Ophthalmologists were sent a semistructured questionnaire on how they manage glaucoma, their training in glaucoma care, where they practice, their access to equipment for diagnosis and treatment, whether they use protocols and the challenges they face in managing patients with glaucoma.
153/250 ophthalmologists in 80 centres completed questionnaires. Although 79% felt their training was excellent or good, 46% needed more training in glaucoma diagnosis and surgery. All had ophthalmoscopes, 93% had access to applanation tonometers, 81% to visual field analysers and 29% to laser machines (in 19 centres). 3 ophthalmologists had only ophthalmoscopes and schiøtz tonometers. For 85%, a glaucomatous optic disc was the most important feature that would prompt glaucoma work-up. Only 56% routinely performed gonioscopy and 61% used slit-lamp stereoscopic biomicroscopy for disc assessment. Trabeculectomy (with/without antimetabolites) was the only glaucoma surgery performed with one mention of canaloplasty. Poor compliance with medical treatment (78%) and low acceptance of surgery (71%) were their greatest challenges.
This study indicates that a systems-oriented approach is required to enhance ophthalmologist's capability for glaucoma care. Strategies to improve glaucoma management include strengthening poorly equipped centres including provision of lasers and training, and improving patients' awareness and education on glaucoma.
青光眼是一种慢性非传染性疾病,是全球不可逆性失明的主要原因,在尼日利亚是一个公共卫生问题,≥40岁人群中的患病率为5.02%。这项全国性调查的目的是评估尼日利亚眼科医生治疗青光眼的实践模式及其面临的限制因素。
向眼科医生发送了一份半结构化问卷,内容涉及他们如何治疗青光眼、青光眼护理方面的培训、执业地点、获得诊断和治疗设备的情况、是否使用治疗方案以及治疗青光眼患者时面临的挑战。
80个中心的250名眼科医生中有153名完成了问卷。尽管79%的人认为他们的培训优秀或良好,但46%的人需要在青光眼诊断和手术方面接受更多培训。所有医生都有检眼镜,93%的人可以使用压平眼压计,81%的人可以使用视野分析仪,29%的人可以使用激光设备(在19个中心)。3名眼科医生只有检眼镜和施尼茨眼压计。对于85%的人来说,青光眼性视盘是促使进行青光眼检查的最重要特征。只有56%的人常规进行前房角镜检查,61%的人使用裂隙灯立体显微镜进行视盘评估。小梁切除术(使用/不使用抗代谢药物)是唯一进行的青光眼手术,仅提及了一例房角成形术。药物治疗依从性差(78%)和手术接受率低(71%)是他们面临的最大挑战。
本研究表明,需要采取以系统为导向的方法来提高眼科医生治疗青光眼的能力。改善青光眼治疗的策略包括加强设备简陋的中心,包括提供激光设备和培训,以及提高患者对青光眼的认识和教育。