Jung Jae Hyun, Song Gwan Gyu, Ji Jong Dae, Lee Young Ho, Kim Jae-Hoon, Seo Young Ho, Choi Sung Jae
Division of Rheumatology, Department of Internal Medicine, Korea University Guro Hospital, Seoul, Korea.
Division of Rheumatology, Department of Internal Medicine, Korea University Anam Hospital, Seoul, Korea.
Korean J Intern Med. 2018 Jul;33(4):815-822. doi: 10.3904/kjim.2016.062. Epub 2016 Oct 12.
BACKGROUND/AIMS: We performed this study to investigate associations between metabolic syndrome, chronic kidney disease (CKD), and gout.
We reviewed the medical records of 151 patients with gout at the Department of Rheumatology in Korea University Ansan Hospital. The following measures were examined: waist circumference, blood pressure, alcohol consumption, and levels of triglyceride, high density lipoprotein cholesterol, fasting serum glucose, serum uric acid (SUA), creatinine, insulin, and C-peptide. We assessed metabolic syndrome by the homeostasis model assessment of insulin resistance (HOMA-IR) index and renal function by the Modification of Diet in Renal Disease equation; patients were classified according to World Health Organization Asia-Pacific obesity criteria.
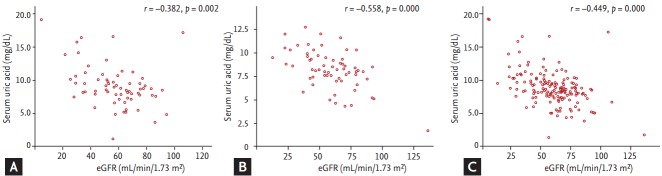
The prevalence of metabolic syndrome in gout patients (50.8%) was higher than in non-gout patients. The mean SUA level was significantly higher in gout patients with metabolic syndrome (9.13 ± 3.15 mg/dL) than in gout patients without metabolic syndrome (8.14 ± 2.07 mg/dL). The mean SUA level was also significantly higher in patients with gout and CKD (9.55 ± 2.86 mg/dL) than in patients with gout but no CKD (7.74 ± 2.27 mg/dL). In gout patients, HOMA-IR was positively correlated with waist circumference (r = 0.409, p = 0.001).
The prevalence of metabolic syndrome in patients with gout was 50.8%, which is higher than the prevalence in the general Korean population. Hyperuricemia in gout patients was correlated with metabolic syndrome and CKD. Insulin resistance may provide clues to better understand the relationship between metabolic syndrome, CKD, and gout.
背景/目的:我们开展本研究以调查代谢综合征、慢性肾脏病(CKD)和痛风之间的关联。
我们回顾了韩国大学安山医院风湿病科151例痛风患者的病历。检查了以下指标:腰围、血压、饮酒量以及甘油三酯、高密度脂蛋白胆固醇、空腹血糖、血清尿酸(SUA)、肌酐、胰岛素和C肽水平。我们通过胰岛素抵抗稳态模型评估(HOMA-IR)指数评估代谢综合征,并通过肾脏病饮食改良公式评估肾功能;根据世界卫生组织亚太地区肥胖标准对患者进行分类。
痛风患者中代谢综合征的患病率(50.8%)高于非痛风患者。合并代谢综合征的痛风患者的平均SUA水平(9.13±3.15mg/dL)显著高于未合并代谢综合征的痛风患者(8.14±2.07mg/dL)。痛风合并CKD患者的平均SUA水平(9.55±2.86mg/dL)也显著高于痛风但无CKD的患者(7.74±2.27mg/dL)。在痛风患者中,HOMA-IR与腰围呈正相关(r = 0.409,p = 0.001)。
痛风患者中代谢综合征的患病率为50.8%,高于韩国普通人群的患病率。痛风患者的高尿酸血症与代谢综合征和CKD相关。胰岛素抵抗可能为更好地理解代谢综合征、CKD和痛风之间的关系提供线索。