Institute of Epidemiology II, Helmholtz Zentrum München, German Research Center for Environmental Health, Neuherberg, Germany.
German Centre for Cardiovascular Research (DZHK), partner site Munich Heart Alliance, Munich, Germany.
PLoS One. 2016 Oct 12;11(10):e0164688. doi: 10.1371/journal.pone.0164688. eCollection 2016.
The 2013 ACC/AHA guidelines introduced an algorithm for risk assessment of atherosclerotic cardiovascular disease (ASCVD) within 10 years. In Germany, risk assessment with the ESC SCORE is limited to cardiovascular mortality. Applicability of the novel ACC/AHA risk score to the German population has not yet been assessed. We therefore sought to recalibrate and evaluate the ACC/AHA risk score in two German cohorts and to compare it to the ESC SCORE.
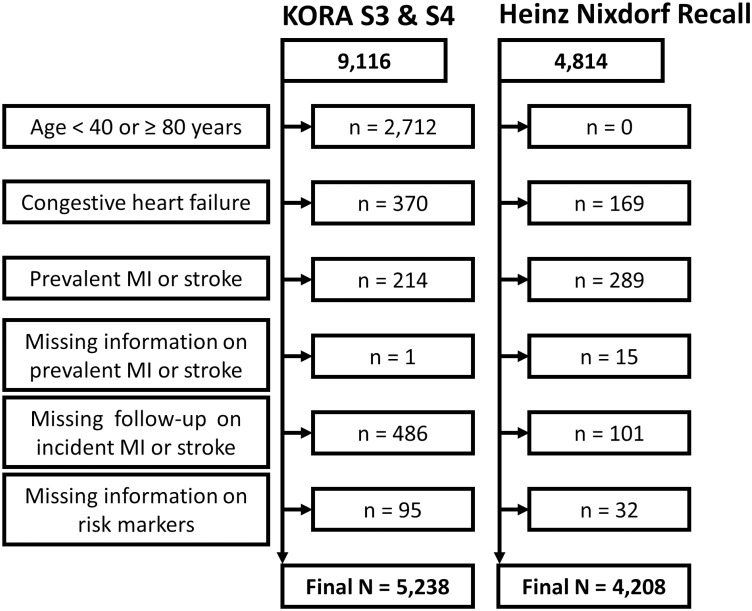
We studied 5,238 participants from the KORA surveys S3 (1994-1995) and S4 (1999-2001) and 4,208 subjects from the Heinz Nixdorf Recall (HNR) Study (2000-2003). There were 383 (7.3%) and 271 (6.4%) first non-fatal or fatal ASCVD events within 10 years in KORA and in HNR, respectively. Risk scores were evaluated in terms of calibration and discrimination performance.
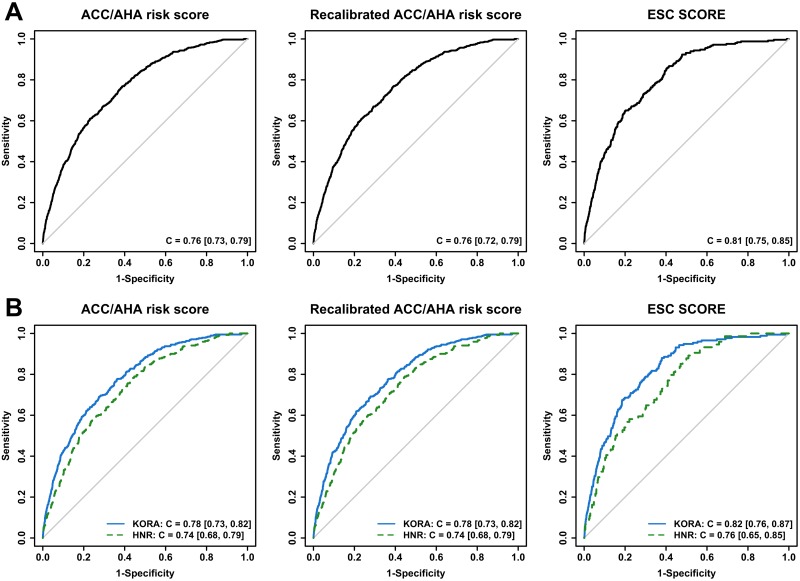
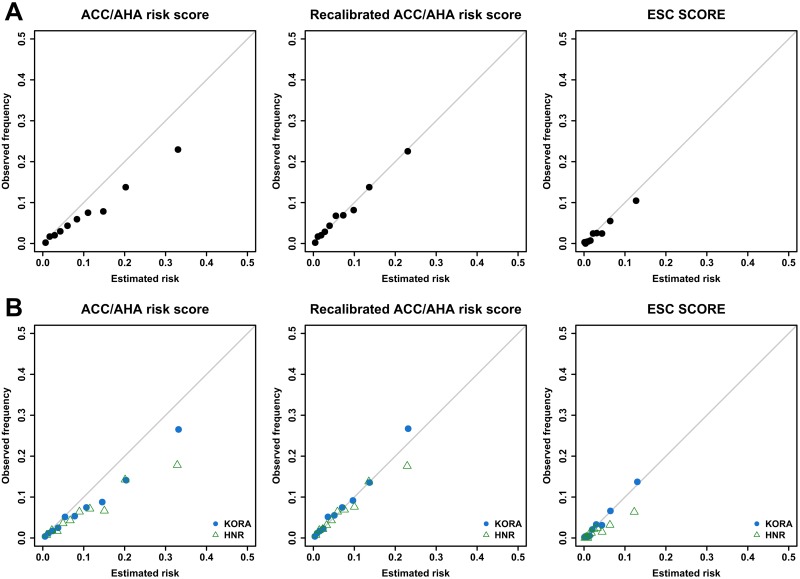
The original ACC/AHA risk score overestimated 10-year ASCVD rates by 37% in KORA and 66% in HNR. After recalibration, miscalibration diminished to 8% underestimation in KORA and 12% overestimation in HNR. Discrimination performance of the ACC/AHA risk score was not affected by the recalibration (KORA: C = 0.78, HNR: C = 0.74). The ESC SCORE overestimated by 5% in KORA and by 85% in HNR. The corresponding C-statistic was 0.82 in KORA and 0.76 in HNR.
The recalibrated ACC/AHA risk score showed strongly improved calibration compared to the original ACC/AHA risk score. Predicting only cardiovascular mortality, discrimination performance of the commonly used ESC SCORE remained somewhat superior to the ACC/AHA risk score. Nevertheless, the recalibrated ACC/AHA risk score may provide a meaningful tool for estimating 10-year risk of fatal and non-fatal cardiovascular disease in Germany.
2013 年 ACC/AHA 指南引入了一种在 10 年内评估动脉粥样硬化性心血管疾病(ASCVD)风险的算法。在德国,ESC SCORE 仅用于评估心血管死亡率的风险。新型 ACC/AHA 风险评分在德国人群中的适用性尚未得到评估。因此,我们试图在两个德国队列中重新校准和评估 ACC/AHA 风险评分,并将其与 ESC SCORE 进行比较。
我们研究了 KORA 调查 S3(1994-1995 年)和 S4(1999-2001 年)的 5238 名参与者和 Heinz Nixdorf 召回研究(HNR)(2000-2003 年)的 4208 名受试者。在 KORA 和 HNR 中,分别有 383(7.3%)和 271(6.4%)名受试者在 10 年内首次发生非致命或致命 ASCVD 事件。我们评估了风险评分的校准和区分性能。
原始的 ACC/AHA 风险评分在 KORA 中高估了 10 年 ASCVD 发生率 37%,在 HNR 中高估了 66%。经过重新校准后,KORA 中低估了 8%,HNR 中高估了 12%。重新校准并未影响 ACC/AHA 风险评分的区分性能(KORA:C=0.78,HNR:C=0.74)。ESC SCORE 在 KORA 中高估了 5%,在 HNR 中高估了 85%。相应的 C 统计量在 KORA 中为 0.82,在 HNR 中为 0.76。
与原始的 ACC/AHA 风险评分相比,重新校准的 ACC/AHA 风险评分显示出了明显的改善。由于 ESC SCORE 仅用于评估心血管死亡率,因此其区分性能仍然略优于 ACC/AHA 风险评分。然而,重新校准的 ACC/AHA 风险评分可能为在德国评估致命和非致命心血管疾病 10 年风险提供了一种有意义的工具。