DeFilippis Andrew P, Young Rebekah, Carrubba Christopher J, McEvoy John W, Budoff Matthew J, Blumenthal Roger S, Kronmal Richard A, McClelland Robyn L, Nasir Khurram, Blaha Michael J
Ann Intern Med. 2015 Feb 17;162(4):266-75. doi: 10.7326/M14-1281.
Accurate risk assessment of atherosclerotic cardiovascular disease (ASCVD) is essential to effectively balance the risks and benefits of therapy for primary prevention.
To compare the calibration and discrimination of the new American Heart Association (AHA) and American College of Cardiology (ACC) ASCVD risk score with alternative risk scores and to explore preventive therapy as a cause of the reported risk overestimation using the AHA-ACC-ASCVD score.
Prospective epidemiologic study of ASCVD.
MESA (Multi-Ethnic Study of Atherosclerosis), a community-based, sex-balanced, multiethnic cohort.
4227 MESA participants aged 50 to 74 years and without diabetes at baseline.
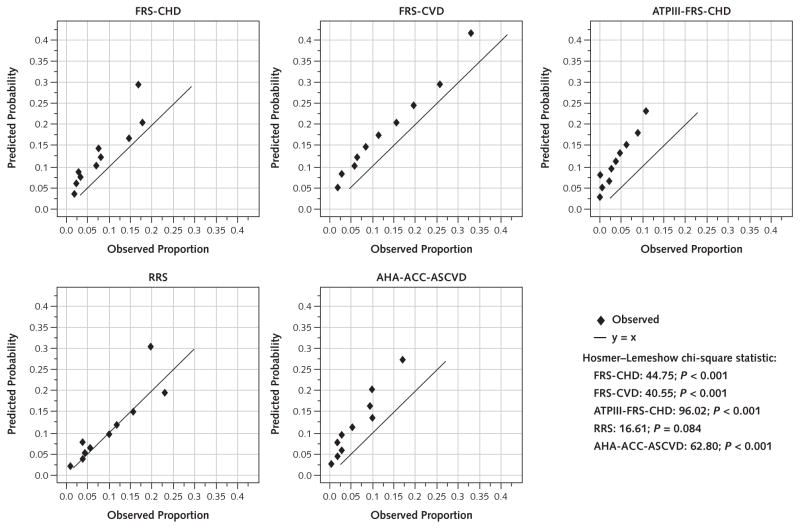
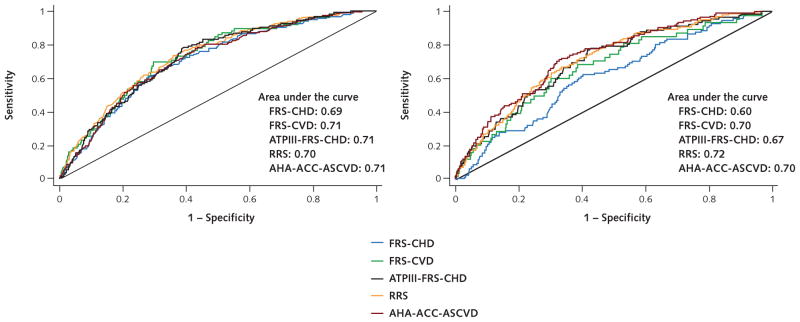
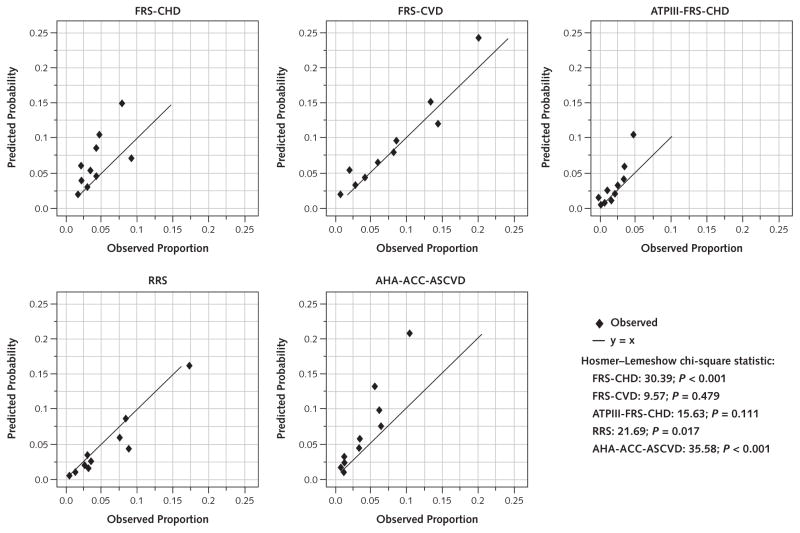
Observed and expected events for the AHA-ACC-ASCVD score were compared with 4 commonly used risk scores-and their respective end points-in MESA after a 10.2-year follow-up.
The new AHA-ACC-ASCVD and 3 older Framingham-based risk scores overestimated cardiovascular events by 37% to 154% in men and 8% to 67% in women. Overestimation was noted throughout the continuum of risk. In contrast, the Reynolds Risk Score overestimated risk by 9% in men but underestimated risk by 21% in women. Aspirin, lipid-lowering or antihypertensive therapy, and interim revascularization did not explain the overestimation.
Comparability of MESA with target populations for primary prevention and possibility of missed events in MESA.
Of the 5 risk scores, 4, including the new AHA-ACC-ASCVD score, showed overestimation of risk (25% to 115%) in a modern, multiethnic cohort without baseline clinical ASCVD. If validated, overestimation of ASCVD risk may have substantial implications for individual patients and the health care system.
National Heart, Lung, and Blood Institute.
准确评估动脉粥样硬化性心血管疾病(ASCVD)的风险对于有效平衡一级预防治疗的风险和益处至关重要。
比较美国心脏协会(AHA)和美国心脏病学会(ACC)新的ASCVD风险评分与其他风险评分的校准和鉴别能力,并探讨使用AHA-ACC-ASCVD评分导致报告的风险高估的预防性治疗原因。
ASCVD的前瞻性流行病学研究。
MESA(动脉粥样硬化多民族研究),一个基于社区、性别均衡、多民族的队列研究。
4227名年龄在50至74岁之间且基线时无糖尿病的MESA参与者。
在10.2年的随访后,将MESA中AHA-ACC-ASCVD评分的观察到的和预期的事件与4种常用风险评分及其各自的终点进行比较。
新的AHA-ACC-ASCVD评分和3种基于弗明汉姆的较旧风险评分在男性中高估心血管事件37%至154%,在女性中高估8%至67%。在整个风险连续体中均观察到高估情况。相比之下,雷诺兹风险评分在男性中高估风险9%,但在女性中低估风险21%。阿司匹林、降脂或降压治疗以及中期血运重建并不能解释这种高估现象。
MESA与一级预防目标人群的可比性以及MESA中可能漏报的事件。
在这5种风险评分中,包括新的AHA-ACC-ASCVD评分在内的4种评分在一个无基线临床ASCVD的现代多民族队列中显示出风险高估(25%至115%)。如果得到验证,ASCVD风险的高估可能对个体患者和医疗保健系统产生重大影响。
国家心肺血液研究所。