Ettner Susan L, M Harwood Jessica, Thalmayer Amber, Ong Michael K, Xu Haiyong, Bresolin Michael J, Wells Kenneth B, Tseng Chi-Hong, Azocar Francisca
Division of General Internal Medicine and Health Services Research, Department of Medicine, David Geffen School of Medicine, University of California, Los Angeles, CA, USA; Department of Health Policy and Management, Fielding School of Public Health, University of California, Los Angeles, CA, USA.
Division of General Internal Medicine and Health Services Research, Department of Medicine, David Geffen School of Medicine, University of California, Los Angeles, CA, USA.
J Health Econ. 2016 Dec;50:131-143. doi: 10.1016/j.jhealeco.2016.09.009. Epub 2016 Sep 30.
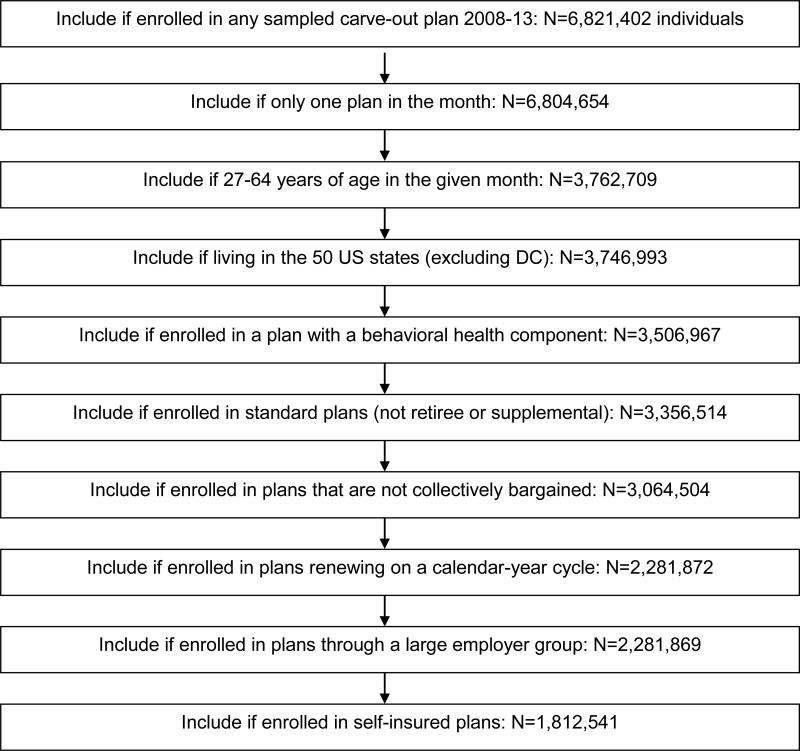
Interrupted time series with and without controls was used to evaluate whether the federal Mental Health Parity and Addiction Equity Act (MHPAEA) and its Interim Final Rule increased the probability of specialty behavioral health treatment and levels of utilization and expenditures among patients receiving treatment. Linked insurance claims, eligibility, plan and employer data from 2008 to 2013 were used to estimate segmented regression analyses, allowing for level and slope changes during the transition (2010) and post-MHPAEA (2011-2013) periods. The sample included 1,812,541 individuals ages 27-64 (49,968,367 person-months) in 10,010 Optum "carve-out" plans. Two-part regression models with Generalized Estimating Equations were used to estimate expenditures by payer and outpatient, intermediate and inpatient service use. We found little evidence that MHPAEA increased utilization significantly, but somewhat more robust evidence that costs shifted from patients to plans. Thus the primary impact of MHPAEA among carve-out enrollees may have been a reduction in patient financial burden.
采用有对照和无对照的中断时间序列设计,评估联邦《精神健康平等与成瘾公平法案》(MHPAEA)及其暂行最终规则是否提高了接受治疗患者获得专科行为健康治疗的可能性、利用水平及支出水平。利用2008年至2013年相关联的保险理赔、资格、保险计划和雇主数据进行分段回归分析,以考量在过渡时期(2010年)及MHPAEA实施后时期(2011 - 2013年)水平和斜率的变化。样本包括Optum公司10,010项“独立核算”计划中年龄在27 - 64岁的1,812,541名个体(49,968,367人月)。使用带有广义估计方程的两部分回归模型,按付款方以及门诊、中级和住院服务使用情况来估计支出。我们发现几乎没有证据表明MHPAEA显著提高了利用率,但有更有力的证据表明成本从患者转移至保险计划。因此,MHPAEA对独立核算参保者的主要影响可能是减轻了患者的经济负担。