Muir Keith W, Ford Gary A, Messow Claudia-Martina, Ford Ian, Murray Alicia, Clifton Andrew, Brown Martin M, Madigan Jeremy, Lenthall Rob, Robertson Fergus, Dixit Anand, Cloud Geoffrey C, Wardlaw Joanna, Freeman Janet, White Philip
Institute of Neuroscience & Psychology, University of Glasgow, Queen Elizabeth University Hospital, Glasgow, UK.
Division of Medical Sciences, Oxford University Hospitals NHS Trust, Oxford University, Oxford, UK.
J Neurol Neurosurg Psychiatry. 2017 Jan;88(1):38-44. doi: 10.1136/jnnp-2016-314117. Epub 2016 Oct 18.
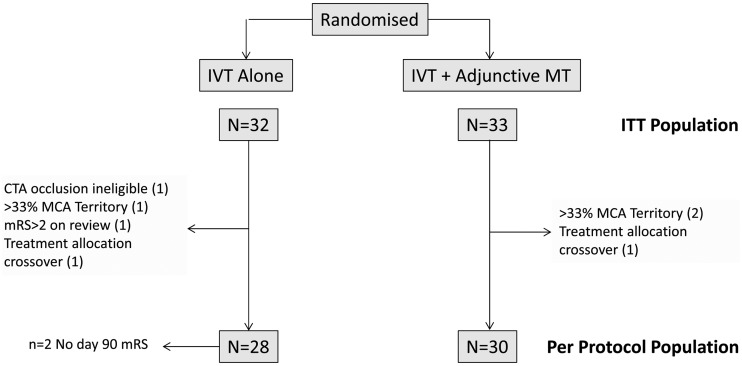
The Pragmatic Ischaemic Thrombectomy Evaluation (PISTE) trial was a multicentre, randomised, controlled clinical trial comparing intravenous thrombolysis (IVT) alone with IVT and adjunctive intra-arterial mechanical thrombectomy (MT) in patients who had acute ischaemic stroke with large artery occlusive anterior circulation stroke confirmed on CT angiography (CTA).
Eligible patients had IVT started within 4.5 hours of stroke symptom onset. Those randomised to additional MT underwent thrombectomy using any Conformité Européene (CE)-marked device, with target interval times for IVT start to arterial puncture of <90 min. The primary outcome was the proportion of patients achieving independence defined by a modified Rankin Scale (mRS) score of 0-2 at day 90.
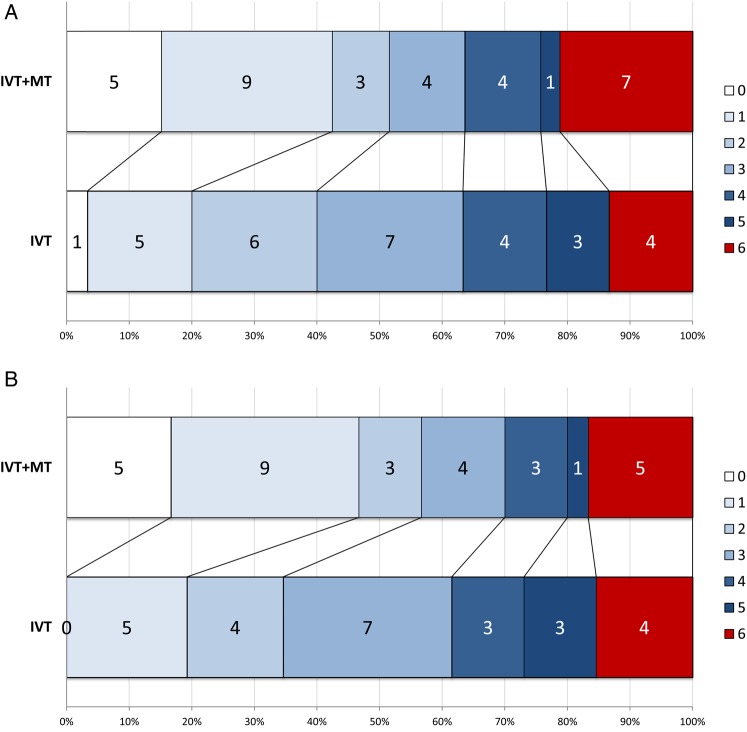
Ten UK centres enrolled 65 patients between April 2013 and April 2015. Median National Institutes of Health Stroke Scale score was 16 (IQR 13-21). Median stroke onset to IVT start was 120 min. In the intention-to-treat analysis, there was no significant difference in disability-free survival at day 90 with MT (absolute difference 11%, adjusted OR 2.12, 95% CI 0.65 to 6.94, p=0.20). Secondary analyses showed significantly greater likelihood of full neurological recovery (mRS 0-1) at day 90 (OR 7.6, 95% CI 1.6 to 37.2, p=0.010). In the per-protocol population (n=58), the primary and most secondary clinical outcomes significantly favoured MT (absolute difference in mRS 0-2 of 22% and adjusted OR 4.9, 95% CI 1.2 to 19.7, p=0.021).
The trial did not find a significant difference between treatment groups for the primary end point. However, the effect size was consistent with published data and across primary and secondary end points. Proceeding as fast as possible to MT after CTA confirmation of large artery occlusion on a background of intravenous alteplase is safe, improves excellent clinical outcomes and, in the per-protocol population, improves disability-free survival.
NCT01745692; Results.
实用性缺血性血栓切除术评估(PISTE)试验是一项多中心、随机、对照临床试验,比较单纯静脉溶栓(IVT)与静脉溶栓联合动脉内机械取栓(MT)在经CT血管造影(CTA)证实为急性缺血性卒中且存在大动脉闭塞的前循环卒中患者中的疗效。
符合条件的患者在卒中症状发作后4.5小时内开始静脉溶栓。随机分配接受额外MT的患者使用任何符合欧洲标准(CE)的设备进行取栓,静脉溶栓开始至动脉穿刺的目标间隔时间<90分钟。主要结局是90天时改良Rankin量表(mRS)评分为0 - 2定义的独立患者比例。
2013年4月至2015年4月期间,英国的10个中心招募了65名患者。美国国立卫生研究院卒中量表评分中位数为16(四分位间距13 - 21)。卒中发作至静脉溶栓开始的中位数为120分钟。在意向性分析中,MT组90天时无残疾生存无显著差异(绝对差异11%,校正比值比2.12,95%置信区间0.65至6.94,p = 0.20)。二次分析显示90天时完全神经功能恢复(mRS 0 - 1)的可能性显著更高(比值比7.6,95%置信区间1.6至37.2,p = 0.010)。在符合方案人群(n = 58)中,主要和大多数次要临床结局显著有利于MT组(mRS 0 - 2的绝对差异为22%,校正比值比4.9,95%置信区间1.2至19.7,p = 0.021)。
该试验未发现治疗组在主要终点上有显著差异。然而,效应大小与已发表数据一致,且在主要和次要终点上均如此。在静脉注射阿替普酶的背景下,CTA证实大动脉闭塞后尽快进行MT是安全的,可改善良好的临床结局,并且在符合方案人群中可提高无残疾生存。
NCT01745692;结果