Gilbert Mark R, Pugh Stephanie L, Aldape Ken, Sorensen A Gregory, Mikkelsen Tom, Penas-Prado Marta, Bokstein Felix, Kwok Young, Lee R Jeffrey, Mehta Minesh
Neuro-Oncology Branch, National Cancer Institute, National Institutes of Health, Bloch Bldg. 82, Rm. 235, 9030 Old George town Road, Bethesda, MD, 20892, USA.
NRG Oncology Statistics and Data Management Center, Philadelphia, PA, USA.
J Neurooncol. 2017 Jan;131(1):193-199. doi: 10.1007/s11060-016-2288-5. Epub 2016 Oct 21.
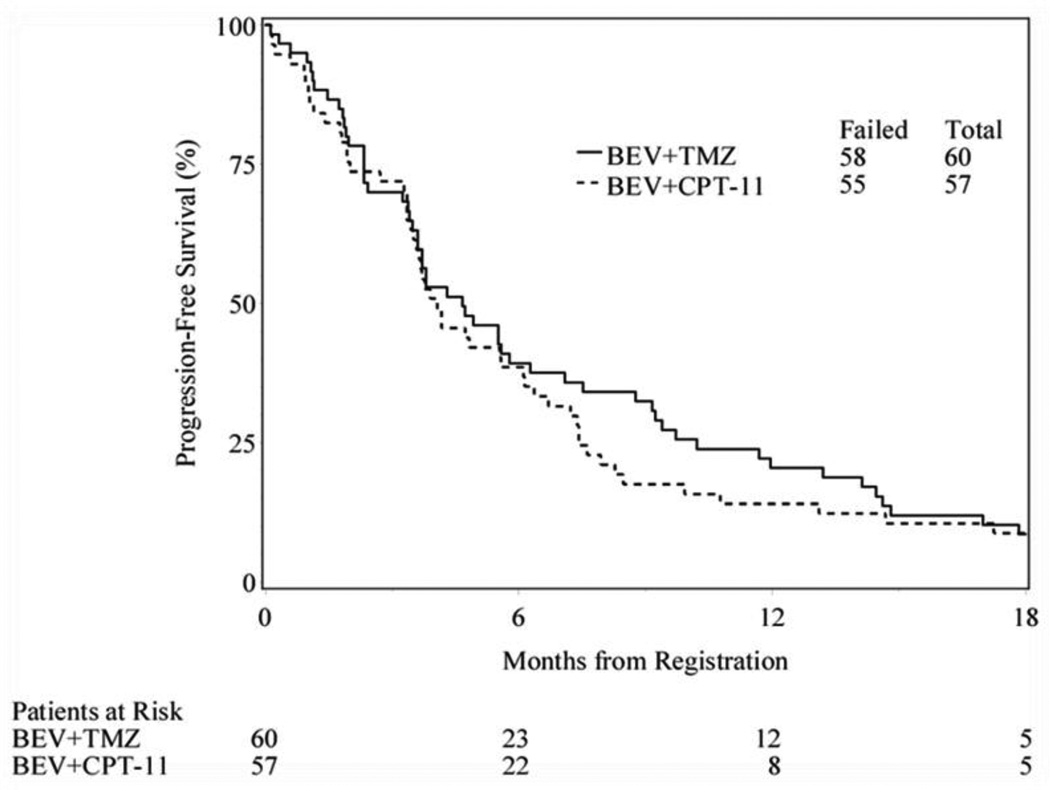
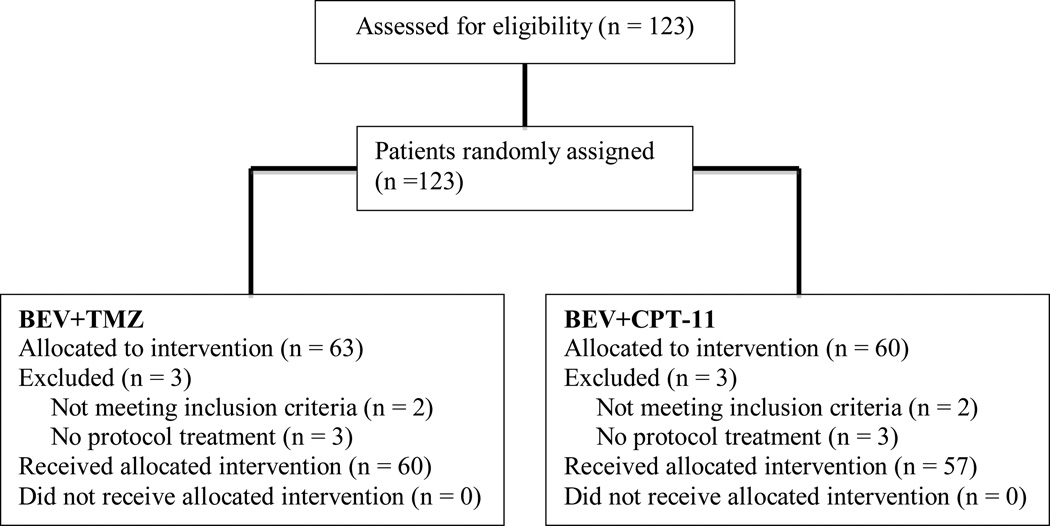
Angiogenesis, a hallmark of glioblastoma, can potentially be targeted by inhibiting the VEGF pathway using bevacizumab, a humanized monoclonal antibody against VEGF-A. This study was designed to determine the efficacy and safety of these regimens in the cooperative group setting. Eligibility included age ≥18, recurrent or progressive GBM after standard chemoradiation. Treatment was intravenous bevacizumab 10 mg/kg and either irinotecan (CPT) 125 mg/m every 2 weeks or temozolomide (TMZ) 75-100 mg/m day 1-21 of 28 day cycle. Accrual goal was 57 eligible patients per arm. Primary endpoint was 6 month progression-free survival (6-m PFS); a predetermined rate of ≥35 % to declare efficacy. 60 eligible patients were enrolled on TMZ arm and 57 patients on CPT arm. Median age was 56, median KPS was 80. For TMZ arm, the 6-m-PFS rate was 39 % (23/59); for the CPT arm, the 6-m-PFS rate was 38.6 % (22/57). Objective responses: TMZ arm had 2 (3 %) CR, 9 (16 %) PR; CPT arm had 2 (4 %) CR, 13 (24 %) PR. Overall there was moderate toxicity: TMZ arm with 33 (55 %) grade 3, 11 (18 %) grade 4, and 1 (2 %) grade 5 (fatal) toxicities; CPT arm had 22 (39 %) grade 3, 7 (12 %) grade 4, and 3 (5 %) grade 5 toxicities. The 6-m-PFS surpassed the predetermined efficacy threshold for both arms, corroborating the efficacy of bevacizumab and CPT and confirming activity for bevacizumab and protracted TMZ for recurrent/progressive GBM, even after prior temozolomide exposure. Toxicities were within anticipated frequencies with a moderately high rate of venous thrombosis, moderate hypertension and one intracranial hemorrhage.
血管生成是胶质母细胞瘤的一个标志,使用贝伐单抗(一种抗VEGF - A的人源化单克隆抗体)抑制VEGF途径可能是一种靶向治疗方法。本研究旨在确定这些方案在协作组环境中的疗效和安全性。入选标准包括年龄≥18岁、标准放化疗后复发或进展的胶质母细胞瘤。治疗方案为静脉注射贝伐单抗10mg/kg,每2周联合伊立替康(CPT)125mg/m²或替莫唑胺(TMZ)75 - 100mg/m²,给药周期为28天,第1 - 21天用药。每组的入组目标是57例符合条件的患者。主要终点是6个月无进展生存期(6 - m PFS);预定有效率≥35%才能宣布有效。替莫唑胺组入组60例符合条件的患者,伊立替康组入组57例患者。中位年龄为56岁,中位KPS为80。替莫唑胺组的6 - m PFS率为39%(23/59);伊立替康组的6 - m PFS率为38.6%(22/57)。客观缓解情况:替莫唑胺组有2例(3%)完全缓解(CR),9例(16%)部分缓解(PR);伊立替康组有2例(4%)CR,13例(24%)PR。总体毒性为中度:替莫唑胺组有33例(55%)3级毒性反应,11例(18%)4级毒性反应,1例(2%)5级(致命)毒性反应;伊立替康组有22例(39%)3级毒性反应,7例(12%)4级毒性反应,3例(5%)5级毒性反应。两组的6 - m PFS均超过了预定的疗效阈值,证实了贝伐单抗和伊立替康的疗效,并确认了贝伐单抗和延长使用替莫唑胺对复发/进展性胶质母细胞瘤的活性,即使在先前使用过替莫唑胺的情况下也是如此。毒性反应在预期频率范围内,静脉血栓形成率中等偏高,有中度高血压和1例颅内出血。